

On May 25, 2024, at the 13th Shanghai Jiao Tong University Vascular Disease Forum (SJVF 2024), Professor Lu Xinwu from the Department of Vascular Surgery of the Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, shared the possible problems that may arise in the process of intraluminal reconstruction of the visceral branches of thoracic and abdominal aortic coarctation aneurysms, as well as some of the reflections of his clinical treatment.
Overview
The use of endoluminal repair (EVAR) was first reported by Argentine surgeon Parodi in 1991. Only about 40% of patients with aneurysms are suitable for EVAR; the neck of the aneurysm is short, or the aneurysm involves important visceral arterial openings. 1996 Park reported two cases of open-window endoluminal septal treatment of AAA, which achieved endoluminal reconstruction of the celiac trunk, superior mesenteric artery and right renal artery. Until today, endoluminal reconstruction of visceral arteries is still a major hot topic in the clinic.
Stents currently available for visceral reconstruction
Currently, there are many stents used for endoluminal reconstruction of visceral arteries, and most of the stents available in domestic clinics today are still customized branch stents, which are expensive and have a long production cycle. Therefore, physician-adapted stents through preoperative measurements or 3D printing technology are the choice of many clinicians.
Thoracoabdominal aortic aneurysm outcomes
For the treatment of thoracic and abdominal aortic aneurysms, thousands of cases in large overseas centers have confirmed the safety and efficacy of window/branching endoluminal repair techniques, and the early and mid-term follow-up results are satisfactory. However, the management of aortic coarctation and aortic aneurysm is still different. Data show that 20% to 60% of aortic coarctation develops into a coarctation aneurysm, 18% of patients rupture and require aggressive treatment, and the average rate of aortic diameter growth in chronic type B coarctation is 7.1 mm/year.
Treatment of entrapments (aneurysms) involving visceral arteries
Treatment of aneurysms involving visceral arteries is now gradually moving from physician-adapted to commercialized instruments. Aneurysms generally have some room for maneuver, and the real technical pain point is how to superselect into the visceral artery. In addition, entrapments (aneurysms) involving visceral arteries have their own characteristics: a narrow true lumen, a stiff lining, and the presence of arterial openings originating from the false lumen.
Endoluminal treatment modalities for chronic aortic coarctation (aneurysm)
True intracavity restoration
Parallel Stands
Advantages: flexible combinations; suitable for a wide range of anatomies; suitable for emergencies and selective operations.
Strengths: Complex anatomic conditions require adequate evaluation; widely used for aortic coarctation aneurysms.
Advantage: single lumen, creating a larger lumen structure.
Advantages: avoids excessive coverage of the true lumen of the aorta; reduces the risk of spinal cord ischemia; a complementary and adjunctive therapeutic measure.
True-False-True
Advantage: utilization of false cavity space.
Case Sharing
Case information (male, 56 years old)
The main complaint:Lower abdominal discomfort for 2 months.
History of present illness:TEVAR for aortic coarctation in 2014; TEVAR again in 2015 to treat endoleak and seal LSA.
Body check:God is clear, expiration is flat, abdomen is soft, bowel sounds are normal, light pressure pain in the right lower abdomen without rebound pain, arterial pulsations in the extremities are normal, NS (-).
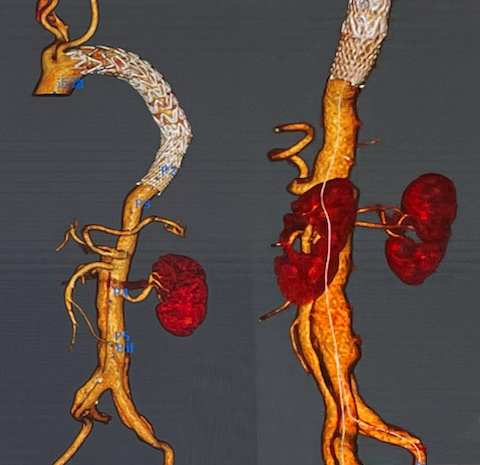
CTA:Abdominal aortic coarctation involving both iliacs, the right kidney as a false lumen feeder, and an aneurysm of the iliac artery coarctation.
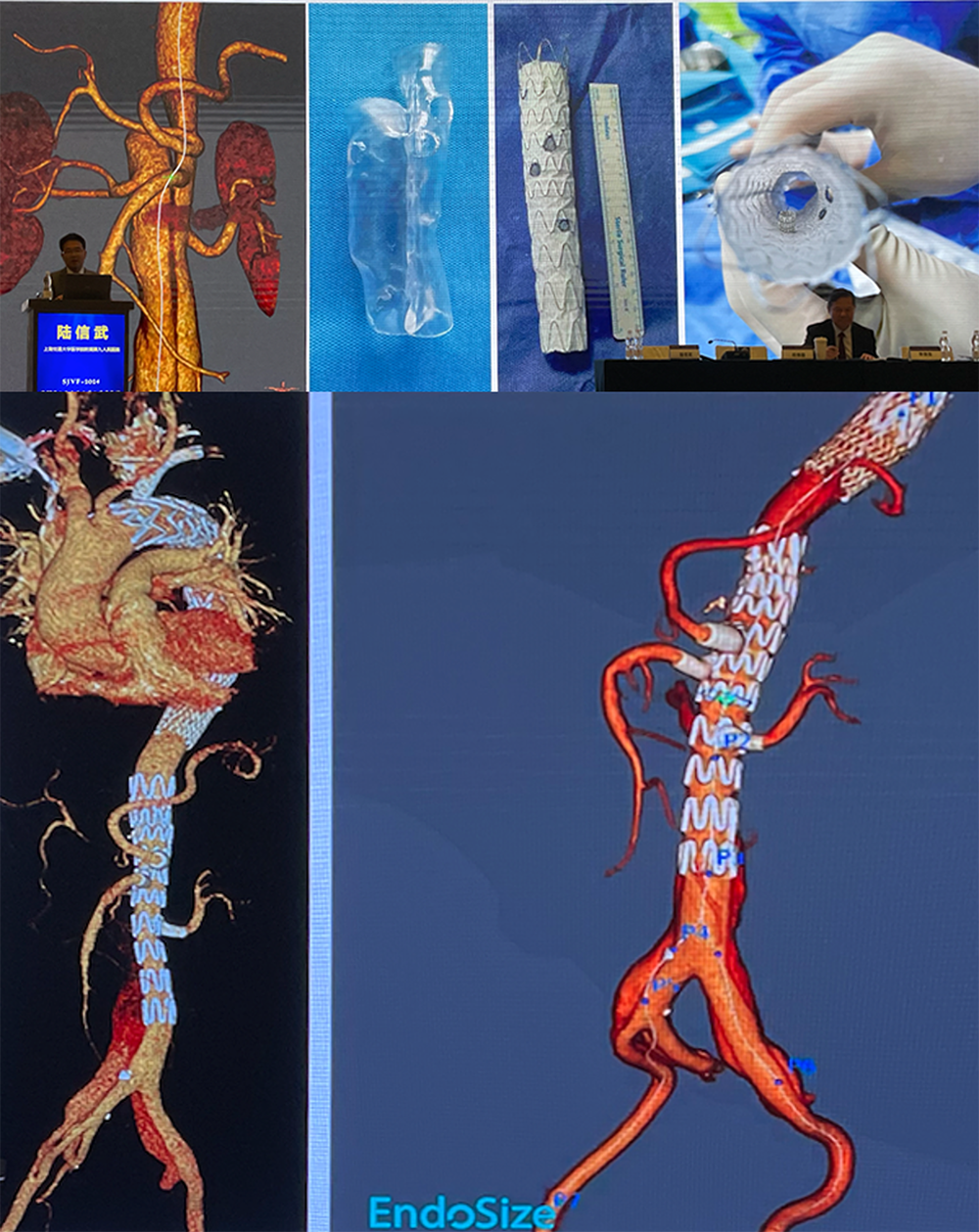
Surgical Strategies: Proposed 3D printing-assisted extracorporeal open-window TEVAR surgery.
Surgical procedure
Surgical Procedure:Based on the preoperative CTA images, an anatomical model was created by 3D printing technology, and accordingly, extracorporeal windowing was implemented at the corresponding position of the main stent. Intraoperatively, the LSA was opened by the in situ windowing technique; then after the release of the main stent, the right intrarenal branch guidewire was dislodged, and the right renal opening was poorly aligned, preventing one-stage reconstruction of the right kidney. A second-stage operation was performed at 1 month later for right renal artery reconstruction by in situ opening, left iliac artery diversion, and right iliac artery embolization.
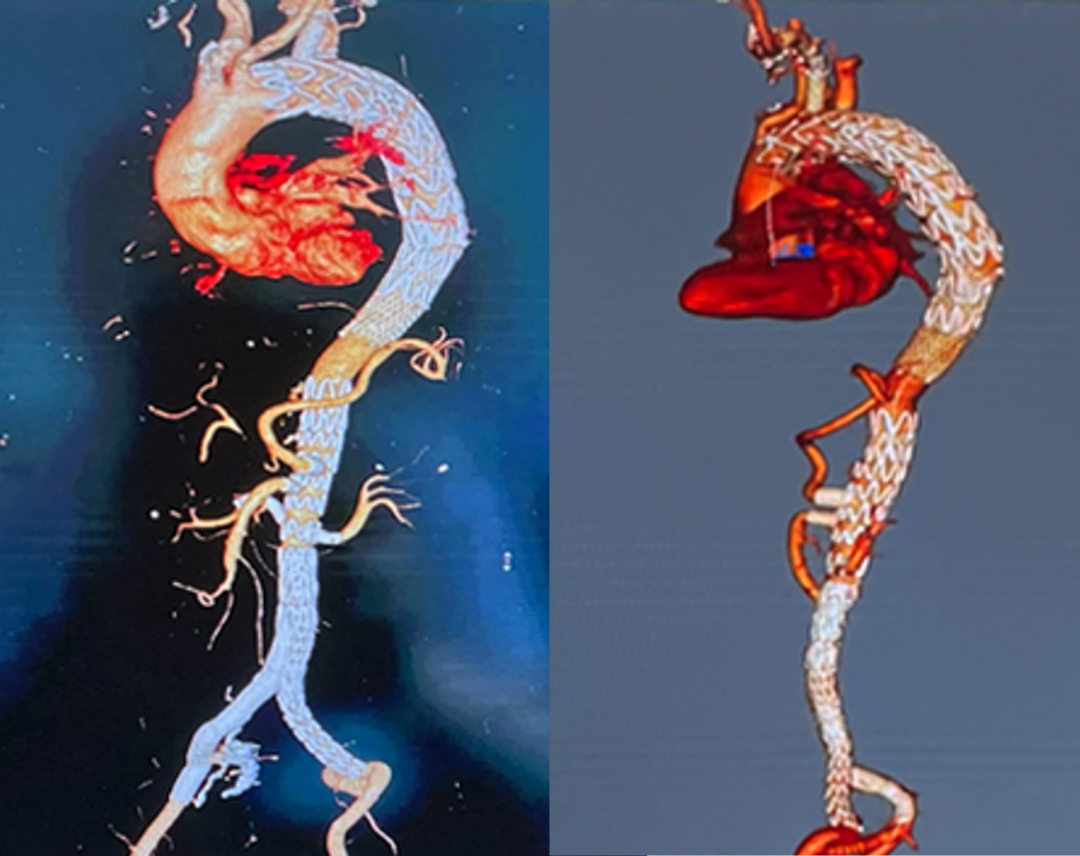
CTA was followed up at 6 months postoperatively:The bracket is in good shape with no internal leaks.
Problems and thoughts on reconstruction of entrapped (aneurysmal) visceral arteries
Currently, the main clinical problems for visceral artery reconstruction of entrapped aneurysms include: the problem of the visceral artery opening into the false lumen of the entrapped aneurysm; access to the visceral artery for reconstruction; the problem of selecting instruments for reconstruction of visceral arteries with a diameter of less than 5 mm; the problem of large aneurysms with large diameters of entrapped aneurysms, but with small diameters of true luminal tubing; the problem of leakage in the reconstruction of visceral arteries; and the problem of problems caused by endothelial rupture or dehiscence.
Reprinted from Outpatient
