
From September 12-14, 2024, the 9th China Vascular Conference (CVC 2024) was successfully held at the Chengdu Century City International Convention Center. During the International and Greater China Region Special Session, Professor Yuliya Panteleeva from the Vascular Surgery Department at the Almazov National Medical Research Centre in Russia shared the current status of aortic disease treatment at their center.

Almazov National Medical Research Centre
The Almazov National Medical Research Centre was founded in 1980 by Vladimir Almazov (a cardiologist) and is located in Russia’s second-largest city, St. Petersburg. It has a total of 1,530 beds, including 223 beds in the anesthesia and intensive care units. The Almazov Centre is a leading scientific contributor and healthcare provider in Russia, offering high-tech medical care under mandatory health insurance and fee-for-service programs. It also has one of Russia’s best hybrid operating rooms.
Current Status of Vascular Surgery in Russia and Internationally
With the aging population and increasing life expectancy, comorbidities are also on the rise. Minimizing surgical invasiveness has become essential. At the same time, minimally invasive technologies are evolving, including endovascular, hybrid, and robotic surgery. Thus, the current trend in vascular surgery is gradually shifting toward minimally invasive endovascular and hybrid surgeries.
Current Status of Vascular Surgery at the Almazov Centre
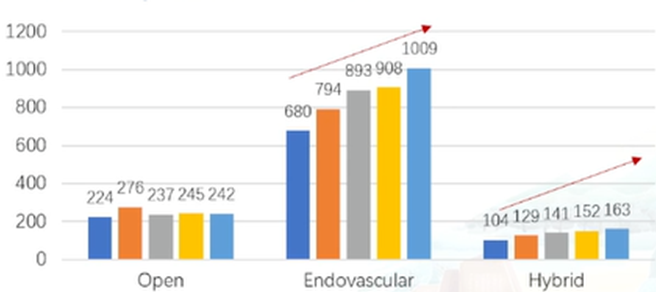
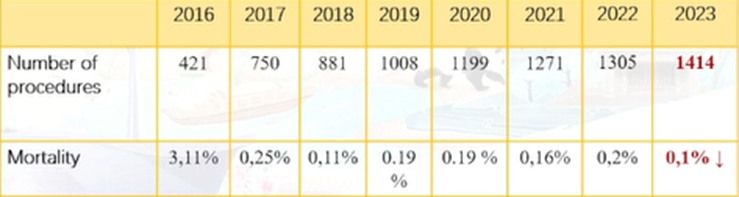
The Almazov Centre performs a comprehensive range of vascular surgeries with the lowest mortality and complication rates. Surgical volume is increasing year by year, with a notable rise in minimally invasive treatments (endovascular and hybrid surgeries), while mortality has been reduced to 0.1%.
Development of Aortic Surgery at the Almazov Centre
•2012: The first EVAR and TEVAR procedures were performed.
•2017: The first ChEVAR procedure was completed to treat a patient with Leriche syndrome using a kissing stent technique.
•2019: Collaborated with Professor Shu Chang to establish an international workshop and completed the first on-table fenestration for endovascular aortic arch repair.
•2021: Completed endovascular aortic arch repair using on-table fenestration and used the CERAB technique to treat a patient with Leriche syndrome.
•2023: Performed endovascular TAAA repair using branched and fenestrated stent-grafts and open TAAA repair combined with ACM (arrhythmogenic cardiomyopathy).
•2024: Used on-table fenestration for TAAA repair and robotic technology for treating aortic diseases.
Annual Aortic Surgery Volume at the Almazov Centre
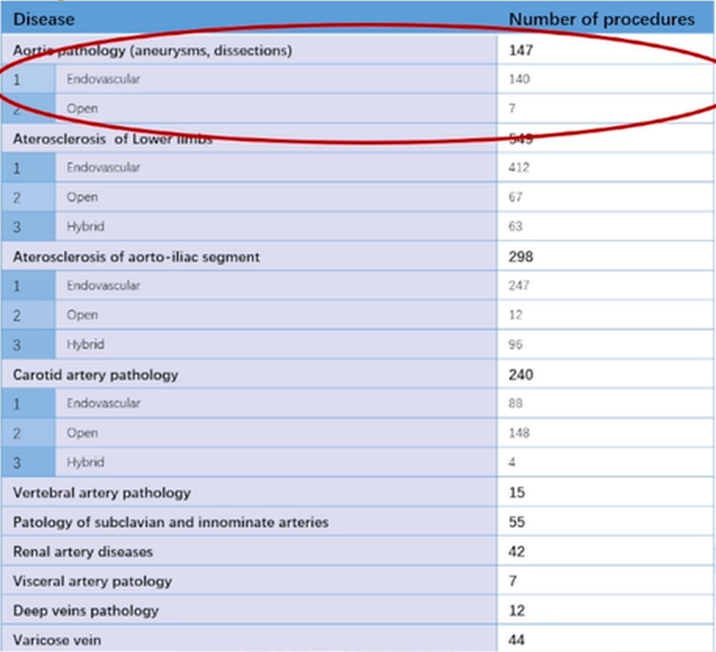
The number of aortic disease surgeries (including aneurysms and dissections) performed annually at the Almazov Centre is steadily increasing. Last year, the center completed 140 endovascular surgeries and 7 open surgeries.
Treatment Strategies for Different Aortic Aneurysms
For aortic aneurysms in different locations, the following strategies are considered:

•Simple Abdominal and Thoracic Aneurysms: Mainly consider endovascular treatment.
•Complex Aneurysms Involving the Brachiocephalic or Visceral Arteries: For high-risk patients, consider endovascular treatment.
Treatment Experience for Aortic Arch Pathology
When treating patients with aortic arch disease, which specialist should be in charge—cardiothoracic surgeons or vascular surgeons? At the Almazov Centre, the patient population managed by each specialty differs:
•Cardiothoracic Surgeons: Perform open and hybrid surgeries (HAR I-III types), primarily for proximal arch and/or ascending aortic aneurysms and dissections, as well as patients with connective tissue disorders and arch pathologies (open surgeries).
•Vascular Surgeons: Perform endovascular and hybrid surgeries (debranching + TEVAR) for thoracic aortic aneurysms/chronic DeBakey type III dissections with a short proximal landing zone (<1.5 cm) and distal arch aneurysms/dissections.
Endovascular Techniques for Aortic Arch Disease
1.Parallel Stent Technique (Chimney)
•Disadvantage: High Type Ia endoleak rate (7.4% to 40%, with an average of 20.1%).
•Advantage: Can be used in emergency situations and for any anatomy.
2.Branched and Fenestrated Stent-Grafts (Not Available in Russia)
•Disadvantage: Expensive, long manufacturing time; requires technical expertise and confidence in implantation.
•Advantage: Customizable and safe for high-risk patients.
3.On-Table Fenestration TEVAR (In-Situ or On-Table Technique)
•Disadvantage: Requires technical expertise.
•Advantage: No manufacturing time needed; cheaper than custom-made stents; can be used in emergencies; lower endoleak risk compared to parallel stents; can be applied to various anatomies using different fenestration methods.
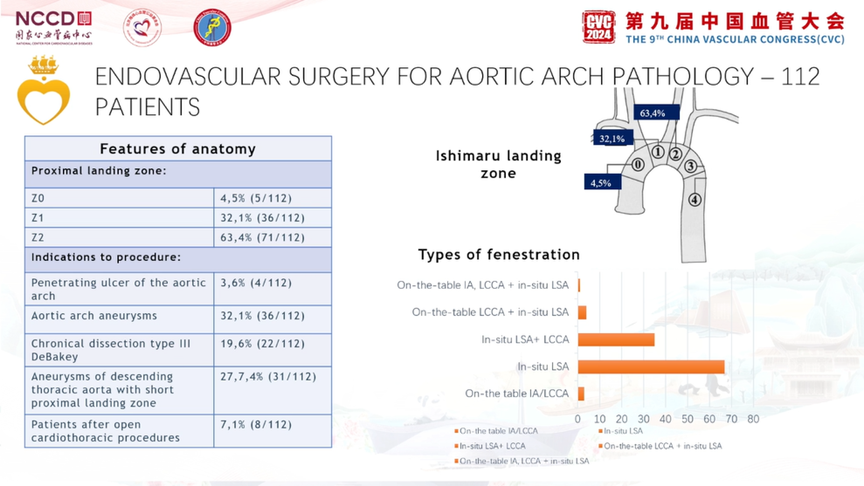
Aortic Arch Endovascular Surgery: 112 Patients
Since 2019, 112 endovascular aortic arch procedures have been performed, with most proximal landing zones in Zone 2. Conditions included aortic arch penetrating ulcers, arch aneurysms, chronic DeBakey III dissections, descending aortic aneurysms with short proximal landing zones, and patients post-cardiothoracic surgery.
The technical success rate was 100%, with a 30-day mortality rate of 0%. Only 3 patients died (1 due to Type Ia endoleak requiring open surgery, 1 due to ruptured abdominal aortic aneurysm, and 1 due to cancer).
Conclusion
Hybrid surgery still has a role in the treatment of aortic arch diseases. It is suitable for:
1.Proximal aortic arch lesions involving the ascending aorta (HAR I-III types).
2.Distal arch lesions combined with:
•Aberrant right subclavian artery.
•LSA originating directly from the aneurysmal sac (high risk of Type II endoleak).
