
Total abdominal aortic occlusion is a rare complication of thoracic aortic dissection (TBAD). Thoracic endovascular aortic repair (TEVAR) is considered the standard treatment for TBAD with malperfusion syndrome. Aortic occlusion may hinder or even prevent the guidance and implantation of stents through the femoral or iliac artery approach. In such cases, immediate surgical intervention may be required to avoid fatal outcomes. During the 9th China Vascular Conference (CVC 2024), held from September 12-14 in Chengdu, Professor Armando De Carvalho Lobato from the Vascular Surgery Institute in São Paulo, Brazil, introduced his innovative endovascular technique called the Lobato Technique (LT), specifically designed for the endovascular treatment of complex thoracic aortic and common iliac artery dissections.

Introduction to the Lobato Technique
Professor Lobato has developed an innovative endovascular technique called the Lobato Technique (LT) for the treatment of complex cases involving TBAD with thoracoabdominal aortic aneurysms (TAAA) and complete true lumen occlusion of the infrarenal abdominal aorta. This technique can be used in emergency situations with off-the-shelf devices, enabling interventionalists to cover the dissection tear, isolate the aneurysmal sac, and simultaneously preserve blood flow to the visceral organs and lower limbs in a single procedure. The LT was developed to overcome anatomical limitations and equipment inadequacies, providing a safe, simple, and cost-effective solution to expand the application of TEVAR.
Detailed Steps of the Lobato Technique
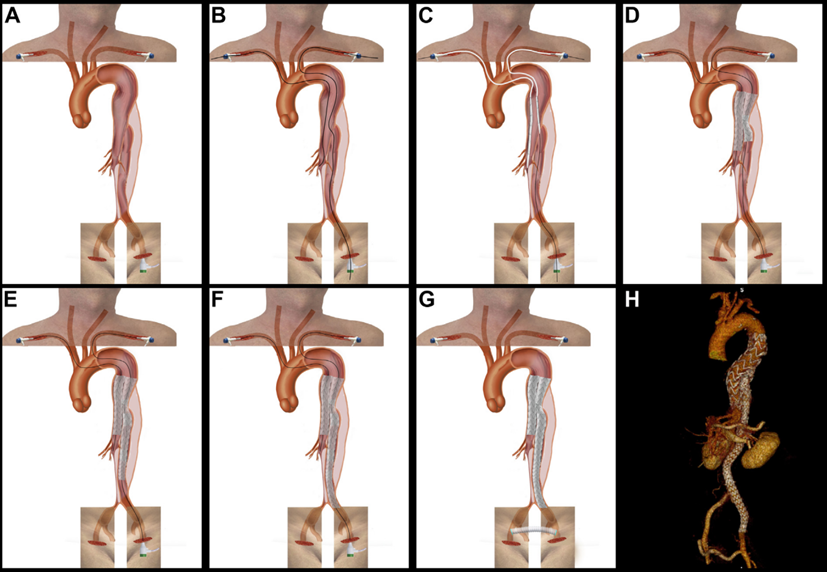
1.Expose and cannulate the left common femoral artery and subclavian artery. A standard guidewire is advanced from the left subclavian artery to the distal left external iliac artery. Another guidewire is introduced from the right subclavian artery into the true lumen of the abdominal aorta.
2.Deploy four stents in sequence:
(1)The first stent is advanced from the right subclavian artery to the celiac trunk.
(2)The second thoracic aortic stent is advanced from the left subclavian artery through the aortic tear from the true lumen into the false lumen.
(3)The third thoracic aortic stent is advanced from the left common femoral artery into the false lumen.
(4)The fourth thoracic aortic stent is advanced from the left common femoral artery into the true lumen at the distal left external iliac artery.
3.Perform a femoral-femoral crossover bypass to restore blood flow to the right limb.
Case Report
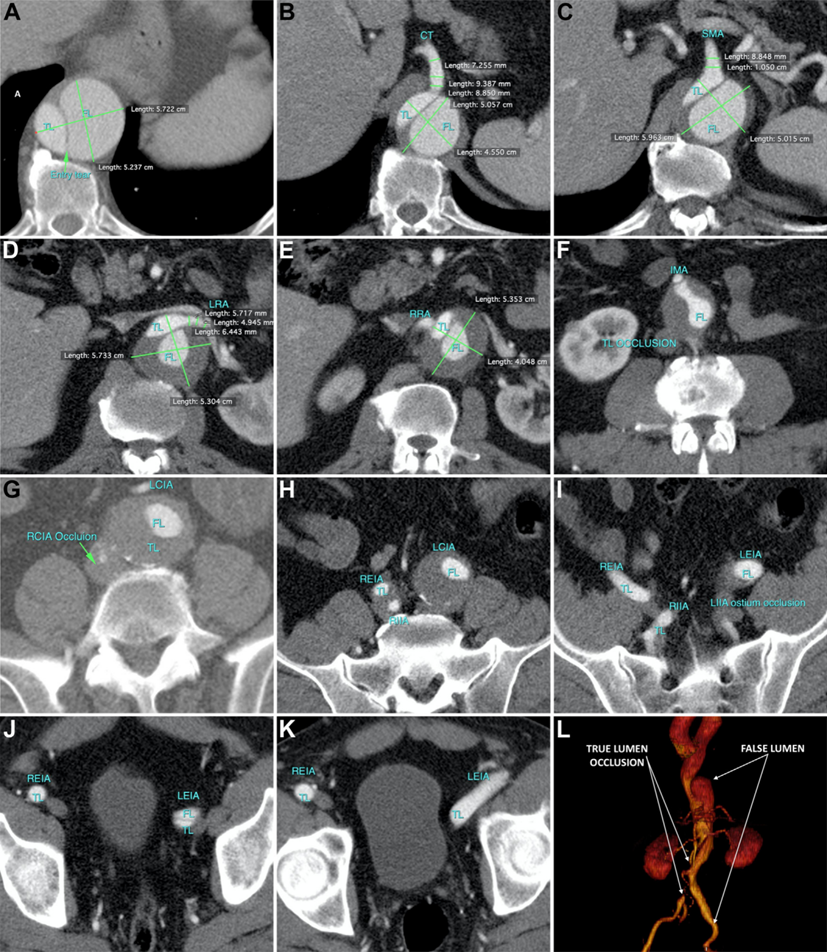
Professor Lobato shared a case report demonstrating the use of this technique in a 63-year-old Caucasian male patient with a history of hypertension who was admitted to a public hospital for acute TBAD. After 12 days of conservative treatment, the patient developed acute malperfusion symptoms in the right lower limb and was transferred to the center. The patient complained of pain, pallor, and numbness in the right lower limb. Emergency CTA revealed complete true lumen collapse of the infrarenal aorta and the right common iliac artery. All visceral arteries originated from the true lumen. At the level of the superior mesenteric artery, the thoracoabdominal aortic aneurysm measured 63 mm in diameter. The infrarenal aortic true lumen and right common iliac artery were completely occluded, but the right internal and external iliac arteries were patent.
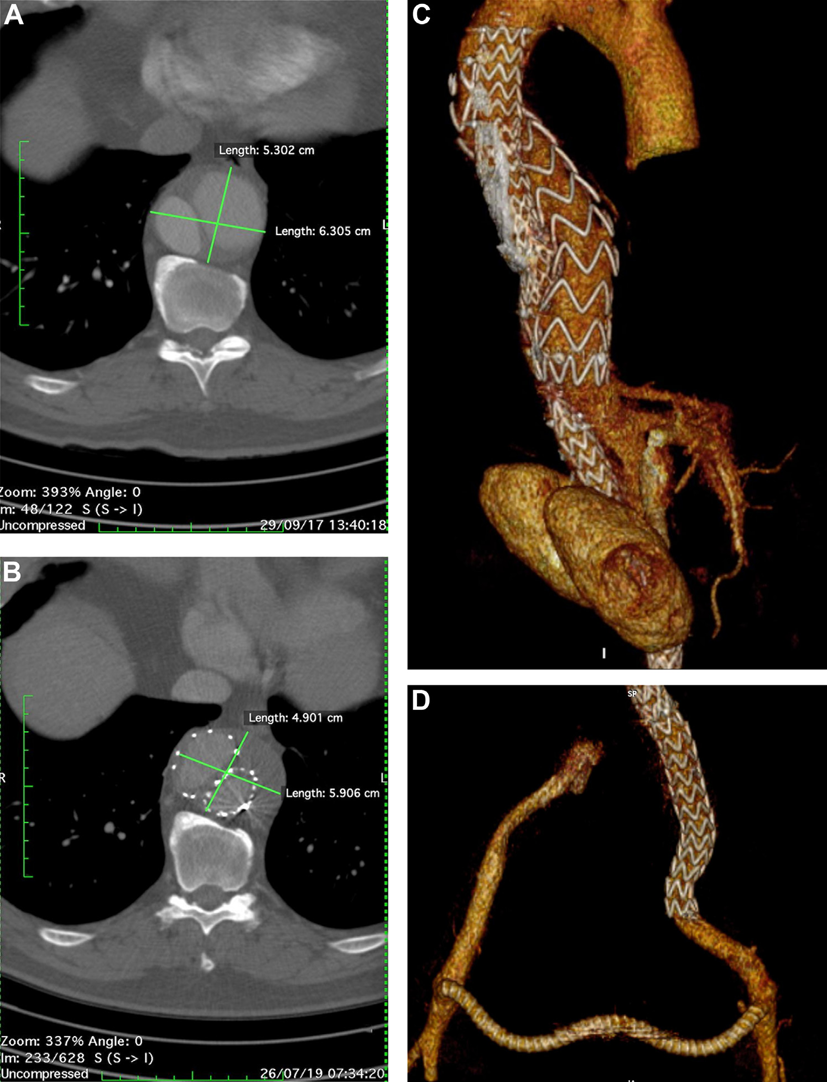
The patient underwent emergency TEVAR under general anesthesia using the Lobato Technique. Intraoperative angiography confirmed restoration of visceral circulation, complete isolation of the TAAA without endoleak, and normal limb perfusion. The procedure and fluoroscopy times were 125 minutes and 26 minutes, respectively. The patient recovered well, and follow-up CTA imaging at three years showed that the aneurysmal sac had shrunk, with patent visceral and lower limb circulation.
Conclusion
The LT aims to overcome anatomical limitations and the constraints of existing devices, providing a safe, simple, and cost-effective method to extend the application of TEVAR for complex TBAD and isolated common iliac artery dissection cases. LT demonstrates potential applicability in TEVAR and EVAR treatment strategies. However, more experience is needed to further refine and expand the use of LT.
