
According to the Stanford Chinese Expert Consensus on the Diagnosis and Treatment of Type B Aortic Coarctation (2022 Edition) [1], reverse-tear Aortic Coarctation (RTAD) due to stent-derived new rupture is one of the most serious complications after TEVAR, which can lead to aortic coarctation rupture, pericardial tamponade, and other serious complications, with an incidence rate of about 2.2%, and the morbidity and mortality rate due to RTAD is The incidence rate is about 2.2%, and the mortality rate due to RTAD is as high as 37.1%.
On November 18, 2023, Prof. Hu Jia's team from the Department of Cardiovascular Surgery, West China Hospital of Sichuan University published a report in the European Heart Journal on the successful use of a novel single-branch intraoperative stent combined with window opening technology to treat a case of RTAD induced by a double chimney stent [2] (click “Read the original article” at the end of the article to view the original article), for the treatment of complex arch vascular lesions. Prof. Hu Jia innovatively used the “Fontus® branching intraoperative stenting system + in situ windowing technique to reconstruct LCCA + ascending aortic replacement” for the first time, which not only effectively treats arch lesions and reconstructs multi-branched vessels, but also reduces the risk of serious complications after open repair of RTAD, which is a new exploration of the treatment of RTAD by open surgery. This is a new exploration of open surgical treatment.
Prof. Hu Jia
Chief Physician, Department of Cardiac Macrovascular Surgery, West China Hospital, Sichuan University, China
Professor / Doctoral Advisor
Case details
Case presentation
Patient male, 46 years old;
The main complaint:Admitted with acute chest pain;
Past history:Stenting of the descending aorta and chimney stenting of the left common carotid artery (LCCA) and left subclavian artery (LSA) were performed 10 years ago;
CTA ancillary tests:Reverse tear Stanford type A aortic coarctation.
Surgical program
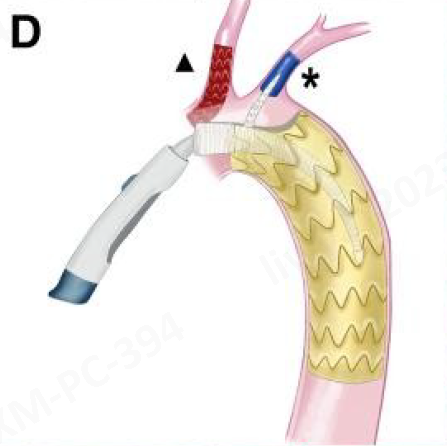
1. According to the CTA results, the patient had undergone stenting of the descending aorta, stenting of the LCCA and LSA “chimney”, and ten years after the operation, she developed a reverse-tear type A aortic coarctation. The patient was symptomatic and urgently needed to be treated by open surgery; Double chimney stent induced reverse tear type A aortic coarctation 2. According to the assessment results, the patient's condition was complex, and he had been implanted with “chimney” stents in the LCCA and LSA in the past. Conventional total aortic arch replacement would have resulted in higher surgical risk, greater vascular damage during stent removal, and extremely difficult distal anastomosis during the operation; 3. Considering that the patient was relatively young, it was decided to complete the reconstruction of the ascending aorta and aortic arch by ascending aortic replacement + elephant trunk stent implantation, but it was still necessary to rebuild the blood flow channels of the LCCA and LSA branches; 4. The Fontus® Branching Intraoperative Stent System (hereinafter referred to as: Fontus® Branching Intraoperative Stent) was selected and opened in situ. The Fontus Branching Intraoperative Stent System adopts a unique single-branching integrated structure, which avoids deep LSA excursion and anastomosis. LSA reconstruction is accomplished by introducing branches into the LSA “chimney” stent. During the operation, an in situ window is opened at the artificial vessel proximal to the Fontus according to the position of the LCCA, and a felt sheet is sewn around the window to reduce the risk of endoleak and complete the LCCA reconstruction.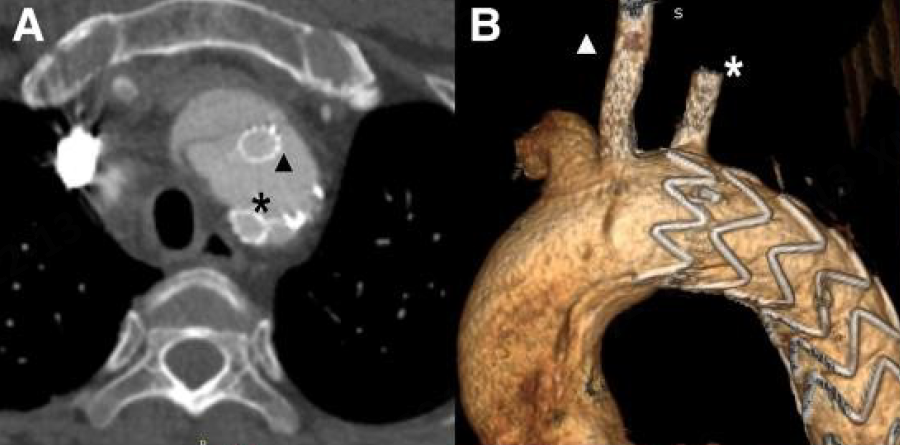
Surgical procedure
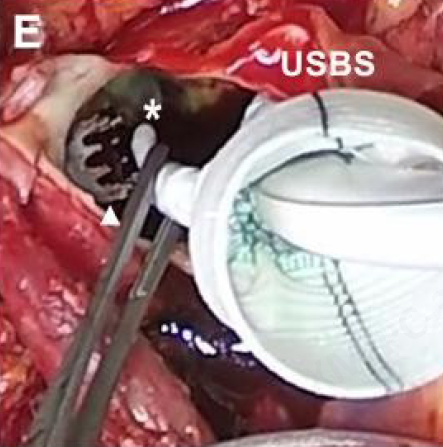
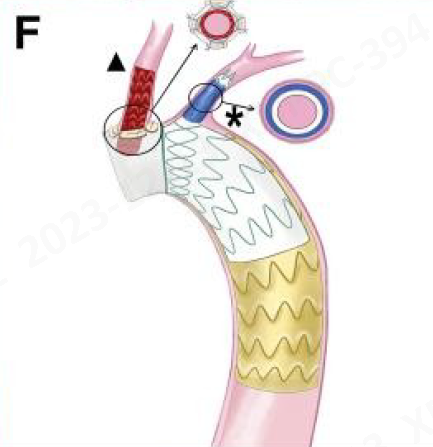
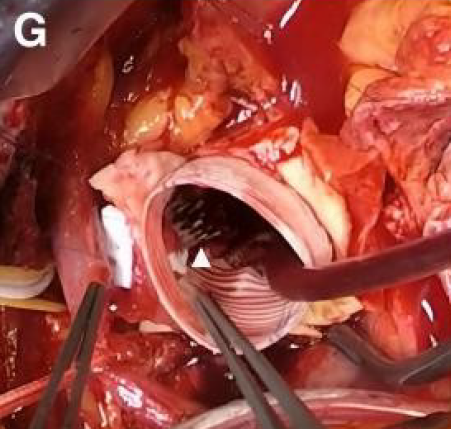
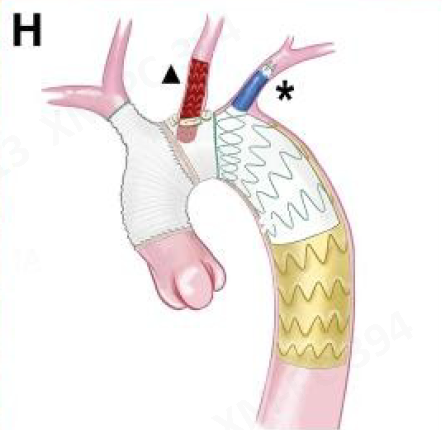
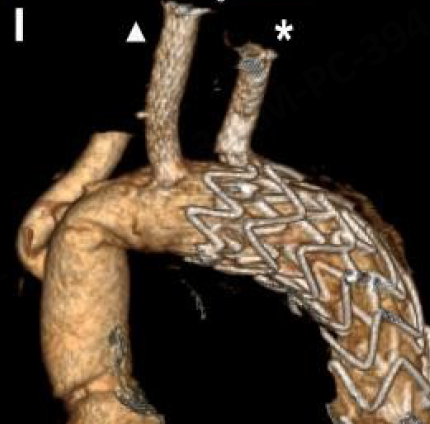
1、Patients were subjected to general anesthesia. During the operation, the chest was opened medianly in the supine position, the innominate artery was freed, and the upper and lower vena cava were cannulated to establish extracorporeal circulation; 2. The ascending aorta and aortic arch were blocked and incised, the distal overlying stent was explored, and the proximal portion of the descending aortic stent and the LSA chimney stent protruding into the arch were trimmed. Trimming LSA Chimney Bracket 3. A Fontus® branching intraoperative stent is placed under direct vision into the descending aorta, and the branch is simultaneously retracted into the LSA chimney stent, and the stent is released by pulling the wire after it has been accurately positioned; Status of the Fontus® branching type intraoperative stent after its introduction Hauling the branch into the LSA chimney bracket 4. Based on the true position of the LCCA, intraoperative in situ windowing was performed at the proximal end of the Fontus® branching type intraoperative stent. After completing an 8-mm-diameter window, the proximal end of the LCCA chimney stent was passed through the window using surgical forceps, and several pieces of felt were used to anastomose the chimney stent to the open window of the Fontus® branching intraoperative stent around the window to reduce the risk of postoperative endoleak; Anastomosis of LCCA chimney stent with Fontus® branching type intraoperative stent proximal to it 5. Perform anastomosis of the proximal end of the stent and the aortic arch of the Fontus® branching type procedure, and then sequentially anastomose the artificial vessel to the proximal end of the stent, the branch of the artificial vessel, and the innominate artery of the Fontus® branching type procedure. After completion of the endocardial artery reconstruction, the aorta was rewarmed and opened, and the heart resumed beating; Anastomosing the proximal end of the Fontus® branching type intraoperative stent to the aortic arch 6, assisted circulation to the stoppage, fish essence protein to neutralize heparin, strict hemostasis was carried out during the operation, the chest was closed layer by layer, the operation process was smooth, and the patient was pushed out of the operating room for postoperative rehabilitation; Postoperative aortic arch morphology 7. Postoperative follow-up CTA showed that the blood flow of the ascending aorta and aortic arch after open surgery was normal, with good morphology, and there was no stent leakage, which made the surgical technique a complete success, and the patient recovered quickly after the surgery. Follow-up CTA 3D reconstruction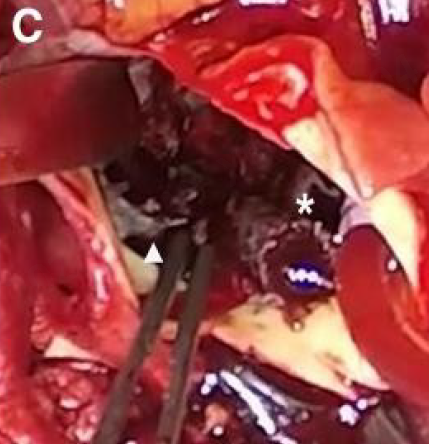
Expert commentary
For the clinical management of patients with reverse tear A aortic dissection (RTAD), the TEVAR procedure has major limitations such as insufficient healthy anchorage area for stenting, difficulty in endoluminal reconstruction of the ascending aorta, and susceptibility to recurrent reverse tearing of the diseased aortic wall due to the inability of the diseased aortic wall to carry the stress of the stent. In contrast, with open surgery, depending on the extent of the involvement of the entrapment, hemodialysis of the diseased vessel can be accomplished by a variety of procedures such as Bentall's procedure, Wheat's procedure, David's procedure, hybridization procedure, elephant trunk stenting and total arch vascular replacement, which reduces the likelihood of new ruptures due to stent origin. For the treatment of this RTAD patient, due to the complexity of the patient's condition, the use of traditional open surgery, there is a high risk of vascular damage from the removal of the stent with intraoperative distal anastomosis difficulty, and the first use of this new surgical technique “Fontus® branching-type intraoperative stenting + in situ windowing technique for reconstruction of the LCCA + ascending aortic replacement “, is an innovation for dealing with complex arch vascular lesions, which not only effectively shortens the operation time and reduces the surgical risk of patients due to long-term off-circulation, but also directly reconstructs the blood flow channel between the LCCA and the LSA, avoids in-depth freeing and anastomosis, effectively reduces the difficulty of the operation, and at the same time effectively reduces the risk of serious complications due to postoperative recurrent rupture of RTAD and pericardial tamponade. It is believed that this new technology will provide more and better treatment options for more patients with reverse-tear type A coarctation in the future.
