Leukemia is a multi-system inflammatory disease of unknown etiology, mainly characterized by recurrent oral ulcers, genital ulcers, uveitis and skin damage, but can also involve peripheral blood vessels, heart, nervous system, gastrointestinal tract, joints, lungs, kidneys and other organs. The disease has a high incidence in Asia, the Middle East and the Mediterranean population, and the scope of the disease coincides with the route of the ancient Silk Road, which is why it has been called the “Silk Road Disease”. Perivalvular leakage and aortic pseudoaneurysms are rare in patients with leukoaraiosis after aortic root replacement, and treatment of postoperative perivalvular leakage combined with infective endocarditis is more difficult.
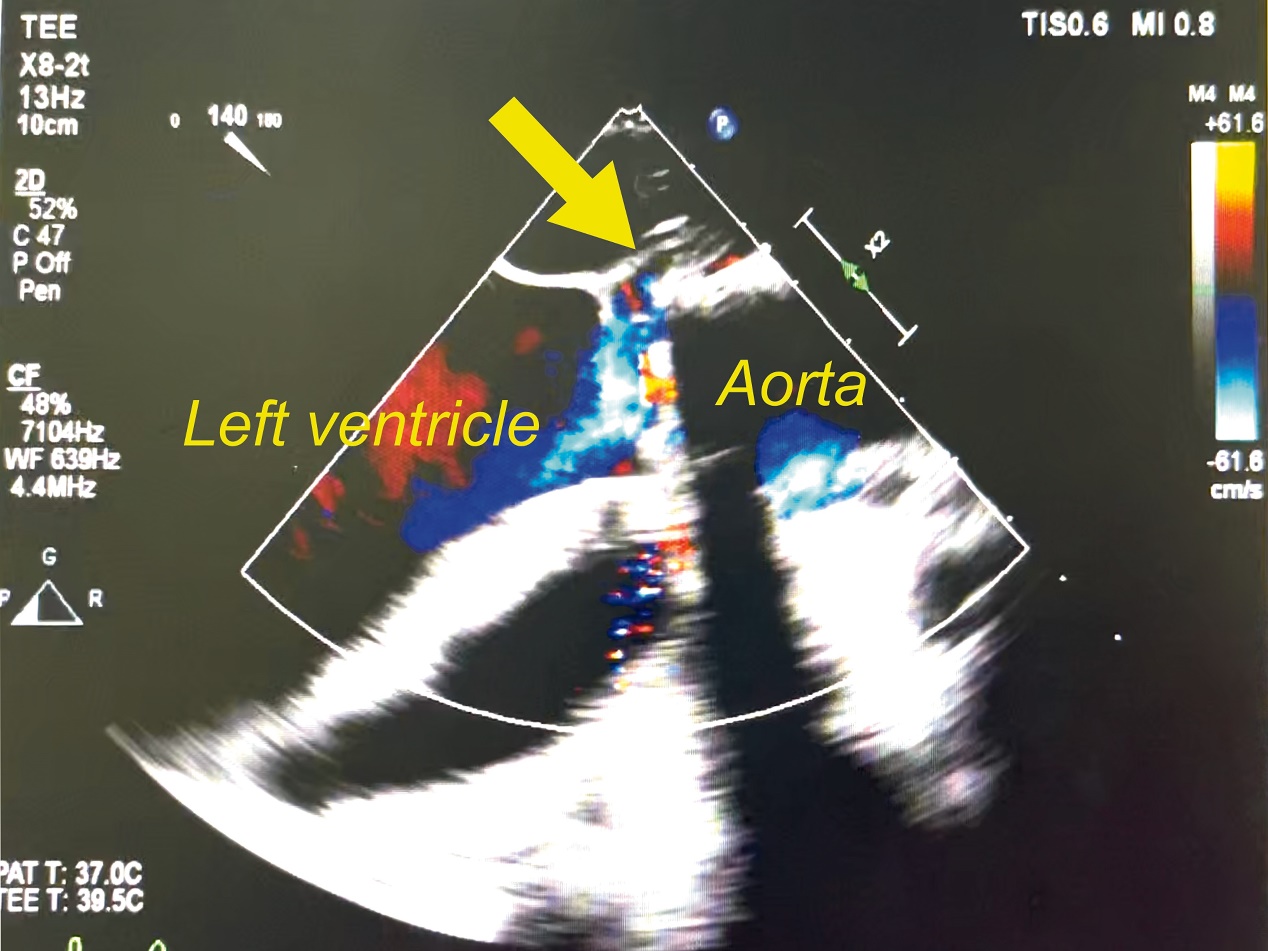
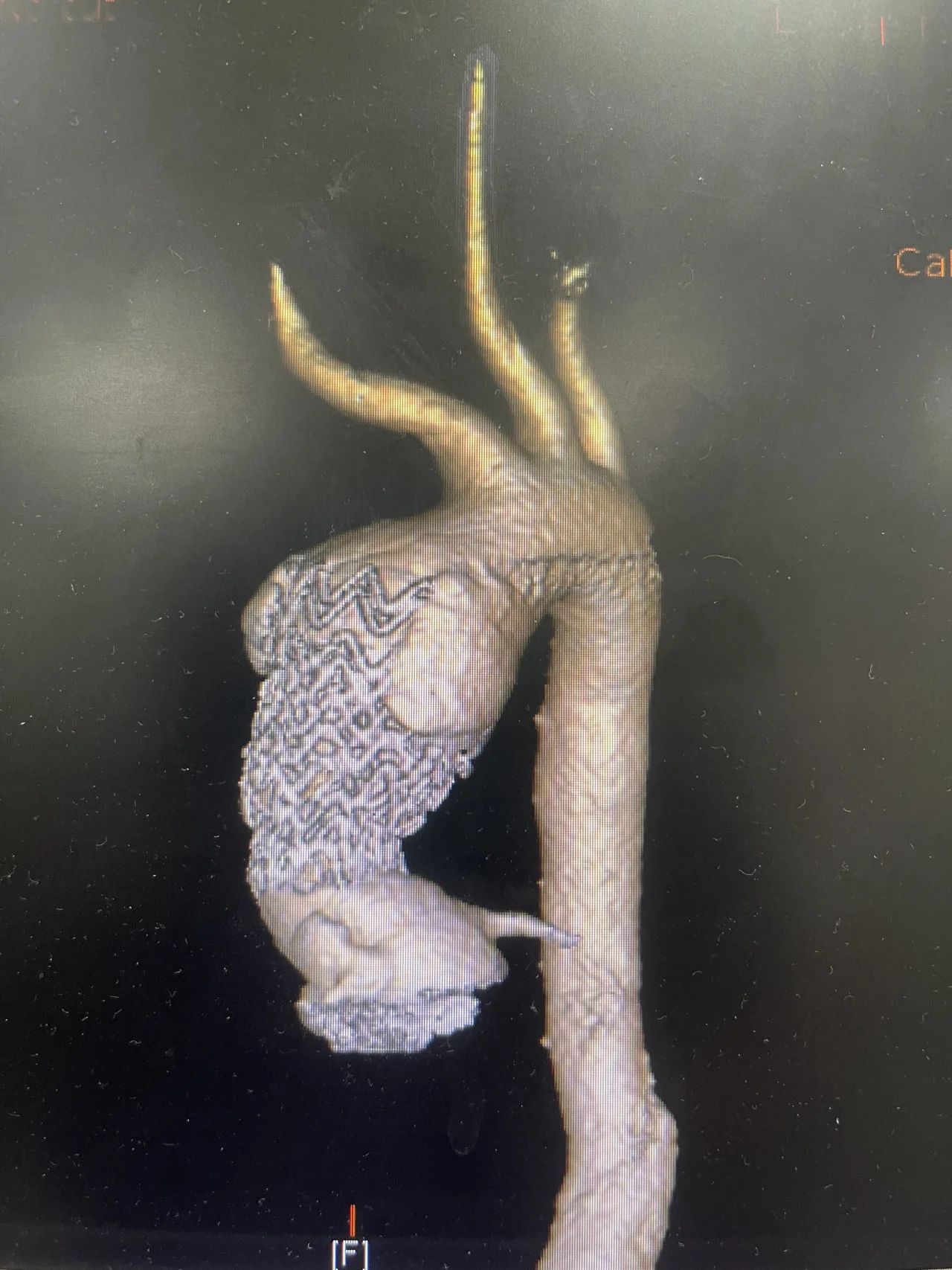
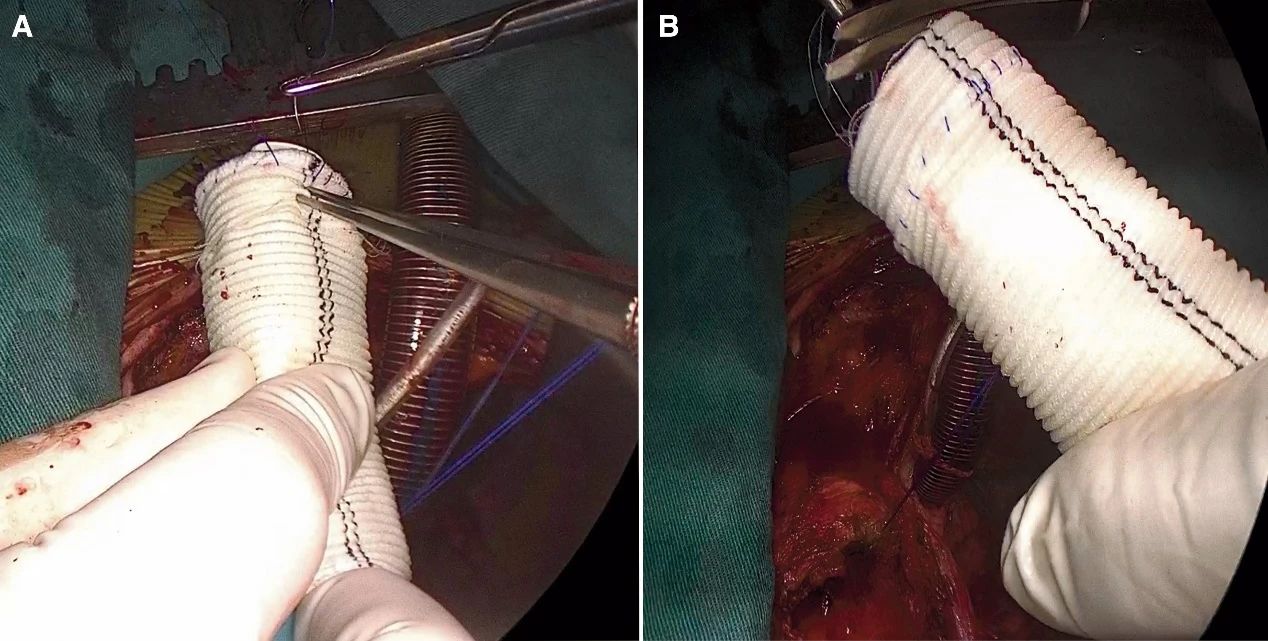
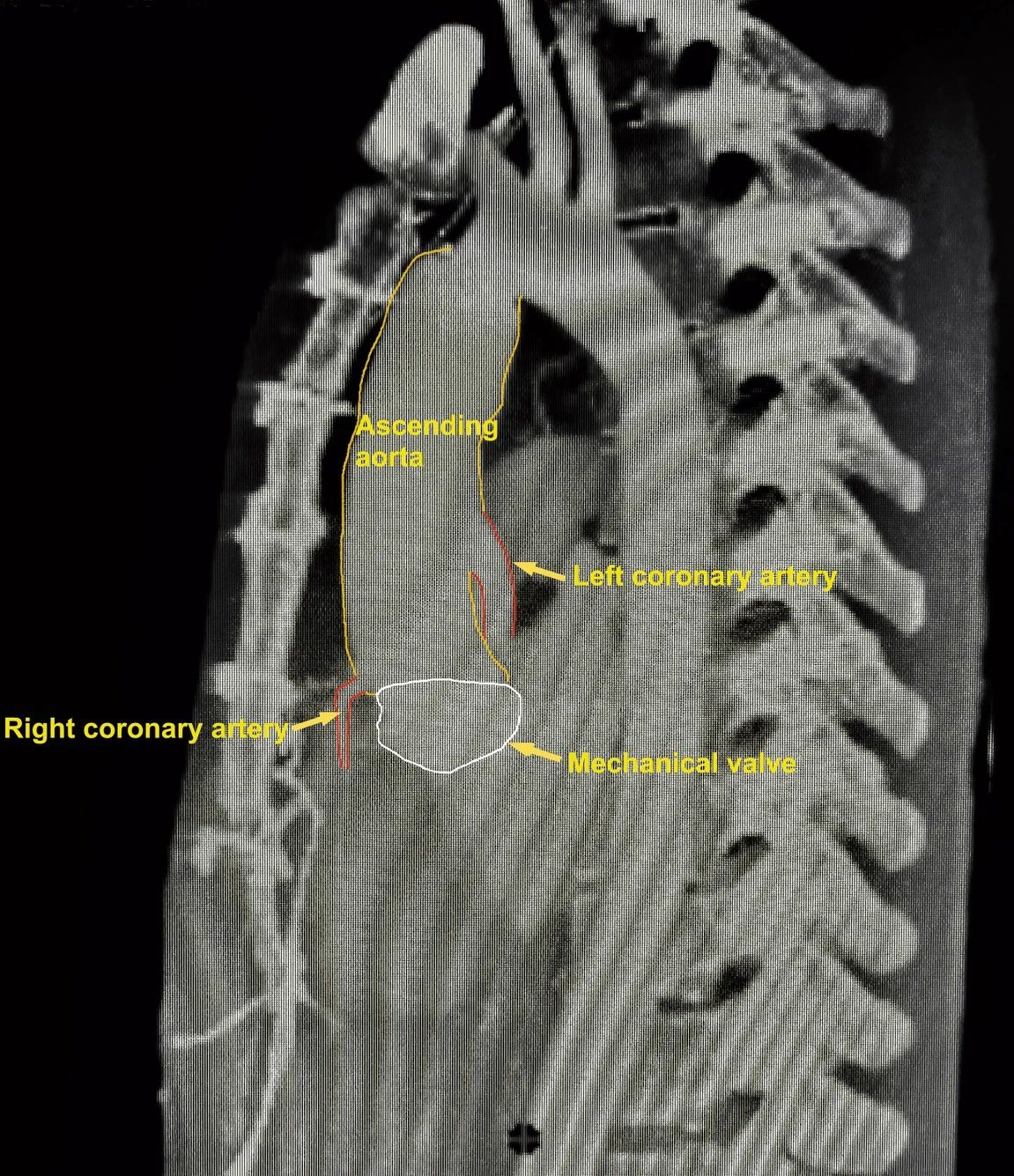
Recently, Prof. Qian Xiangyang's team at Fu Wai Hospital, Chinese Academy of Medical Sciences, published an article in European Heart Journal-Case Report, a sub-journal of EHJ, an international TOP journal, reporting a case of perivalvular leakage and pseudoaneurysm due to leukoaraiosis and infective endocarditis treated by Flanged Bentall, which has made a positive This article provides a new strategy for this type of treatment. Case presentation The patient is a 27-year-old male who presented to the local hospital 5 years ago with exertional dyspnea for 6 months, oral diuretics, and a 5-year history of recurrent oral and genital ulcers. Imaging showed aortic regurgitation and aortic root aneurysm. A Bentall procedure was performed at a local hospital with the implantation of a 20 mm Medtronic ATS mechanical valve and a 26 mm prosthetic vessel. Postoperative electrocardiogram showed complete third degree AV block with a heart rate of approximately 40 beats/minute, but no dizziness or syncope was observed, so a permanent pacemaker was not implanted. Histopathology of the resected tissue showed fibromucoid deformation with leukocyte infiltration, and leukoaraiosis was diagnosed. Oral prednisone (10 mg/day) was administered after the operation, and the patient was found to be normal after 6 months, and the patient discontinued the prednisone on his own. One year after the operation, the patient had a sudden chest, and CT of the thoracic aorta showed a pseudoaneurysm at the distal anastomosis of the ascending aorta, and he underwent percutaneous intraluminal isolation of the ascending aortic laminar stent + temporary pacemaker implantation, with the implantation of two 36 mm aortic laminar stents. Four days after endovascular intervention, the patient developed fever and blood cultures were positive for Streptococcus grass green and oral streptococcus. The temporary pacemaker was removed. Targeted antibiotic therapy was initiated based on drug sensitivity results. Over the next 4 months, the patient's temperature fluctuated between 36°C and 38°C. Laboratory tests showed a white blood cell count of 1.06-8.58*109/L (reference range: 4-10*109/L), C-reactive protein 47-63 mg/L (reference range: 0-8 mg/L)), and an erythrocyte sedimentation rate of 12-36 mm/h (reference range: 0-15 mm/h), and subsequent of blood cultures were negative. Transesophageal echocardiography (Figure 1) showed perivalvular leakage and dysfunction of one side of the mechanical valve leaflet, and aortic CT showed pseudoaneurysm of the ascending aorta and type I endoleak (Figure 2), which was treated surgically after 3 months of anti-inflammatory therapy. Figure 1: Transesophageal echocardiography before the third procedure, arrows indicate areas of perivalvular leakage. Figure 2: CT of the aorta showing pseudoaneurysm of the ascending aorta Surgical procedure Femoral artery cannulation and atrial cannulation were chosen to establish extracorporeal circulation, and the pseudoaneurysm was 6cm*4cm in size with severe periaortic adhesions. After aortic cross-blocking, the aneurysm was incised and the malfunctioning valved conduit was removed. Aortic root replacement was performed using the “petticoat technique” (Flanged Bentall; Figure 3) based on a self-assembled valve prosthesis with a composite graft, in which a 22-mm AP 360 Medtronic mechanical valve was sutured to a 26-mm Maquet prosthesis with ectropion of the edges, and a 26-mm Maquet prosthesis with ectropion of the edges was sutured to a 26-mm Maquet prosthesis. The ectasized prosthesis was then turned back to form a composite valve-prosthesis graft. The edges of the composite prosthesis (5 mm long) were sutured to the aortic annulus using interrupted sutures. Given the tension at the left coronary anastomosis, the left coronary opening was reconstructed preferentially with an 8-mm prosthetic vessel using the Cabrol procedure. The right coronary artery opening was anastomosed end-to-end with the composite prosthetic graft. The distal end of the composite is anastomosed to the transected aortic end using a continuous 4-0 polypropylene suture. Figure 3: Preparation of petticoat-type valve artificial vascular composite grafts. (A) A portion of the vascular graft is turned outward to form a petticoat, and a mechanical valve is sutured to the artificial vessel with continuous 4-0 polypropylene. 、 (B) The petticoat-assembled valve prosthetic vascular composite graft is prepared by flipping the outwardly turned prosthetic vessel back to its original position. A permanent pacemaker was implanted after surgery. Immunosuppression consisted of oral prednisone (1 mg/kg/day) and cyclophosphamide (100 mg/day); cultures of aortic tissues and grafts were negative; antibiotic therapy (ceftriaxone) was continued for 8 weeks; and cardiovascular examination was normal with class I cardiac function after 3 months. CT scans were normal during follow-up (Figure 4). Case Reveal Infective endocarditis is a rare complication of leukoaraiosis. Surgical treatment of aortic valve insufficiency due to leukoaraiosis is characterized by a high incidence of perivalvular leakage, a high rate of reoperation, and a high rate of mortality, and a concomitant infective endocarditis further increases the difficulty and risk of the treatment; therefore, patient education is also crucial, and patients should pay sufficient attention to the disease and cooperate with the treatment. Immunosuppressive therapy should never be discontinued arbitrarily, and it is important to maintain effective immunosuppressive therapy while monitoring serum ESR and CRP levels; however, potential drawbacks are an increased risk of infection and the occurrence of poor tissue healing. In this case, a good balance of targeted antibiotic therapy and appropriate immunosuppressive therapy was achieved, and the pseudoaneurysm occurred after the patient discontinued the medication on his own, caused by a recurrence of leukoaraiosis. In addition, open surgery should be preferred over endovascular stenting for pseudoaneurysms of the ascending aorta, and if the patient did not receive endovascular stenting, she may not have had infective endocarditis; the development of perivalvular leakage may be associated with recurrence of leukoaraiosis and infective endocarditis, and pharmacologic therapy for prosthetic valve endocarditis should be continued for ≥6 weeks, according to the ESC guideline recommendations, with the duration of therapy based on the duration of effective antibiotic therapy on the day one. After the patient's third surgery, targeted antibiotic therapy was continued for 8 weeks and blood cultures were negative during the follow-up period. In this case, the use of the flanged technique (Bentall), based on a self-assembled valve prosthesis with a composite graft, was also a key to success, as the prosthesis had better elasticity, which facilitated the implantation of a larger valve. The patient's aortic annulus, which was only 20 mm in diameter, was implanted with a 22 mm Medtronic AP 360 supra-annular mechanical valve, which increased the effective orifice area of the aorta from 1.3 cm² to 2.1 cm². In leukoaraiosis, where recurrent inflammatory changes cause the aortic annulus and wall to become fragile, the “petticoat” Bentall procedure is ingenious in that the fragile reconstructed aortic annulus is sutured to the prosthetic vascular material rather than directly to the relatively stiff suture ring of the prosthetic valve, which is subject to less tension and fits more tightly, helping to prevent perivalvular leakage. The ring is under less tension and fits more tightly, which helps prevent perivalvular leakage. The “petticoat” of the composite graft reduces tension and vibration of the suture ring throughout the cardiac cycle, thereby reducing the risk of cracking. It also facilitates exposure of the aortic root and hemostasis; short-term results are favorable in the context of the case, but long-term follow-up is needed. Expert Profiles Qian Xiangyang Fu Wai Hospital, Chinese Academy of Medical Sciences, Fu Wai, China