


Data from the CREST and ACT1 studies, controlled studies of large-scale CAS and CEA, were included for patient-level, prespecified, pooled analyses. The primary end point was perioperative death, stroke, or myocardial infarction, or pooling of any ipsilateral stroke within 4 years of randomization. Patients were included as randomized, aged<80 years="">
The final enrollment consisted of 2,544 cases comprising 1,637 CAS and 907 CEAs, all asymptomatic patients<80 years="" of="" age="">
Findings
Primary end point: The pooled incidence of perioperative death, stroke, myocardial infarction, or 4-year ipsilateral stroke was similar between the CEA and CAS groups, at 5.3% and 5.1%, respectively (P = 0.91) (Figure 1).
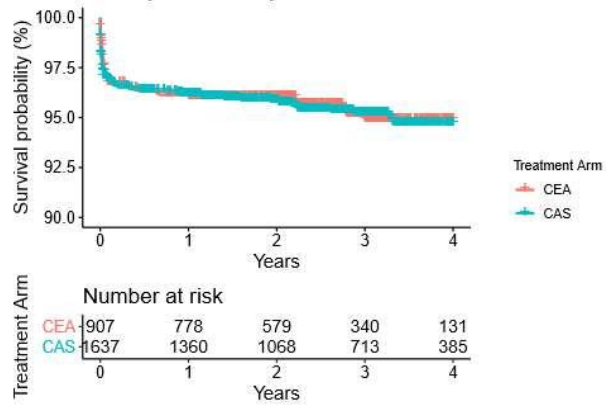
Figure 1. no difference in primary endpoints between CEA and CAS groups
Age subgroups: in the CAS group, there was a difference in risk between age strata (P < 0.0001). <The pooled incidence of perioperative death, stroke, myocardial infarction, or 4-year ipsilateral stroke was significantly lower in the group of patients<65 years="" of="" age="" than="" in="" the="" group="" patients="">
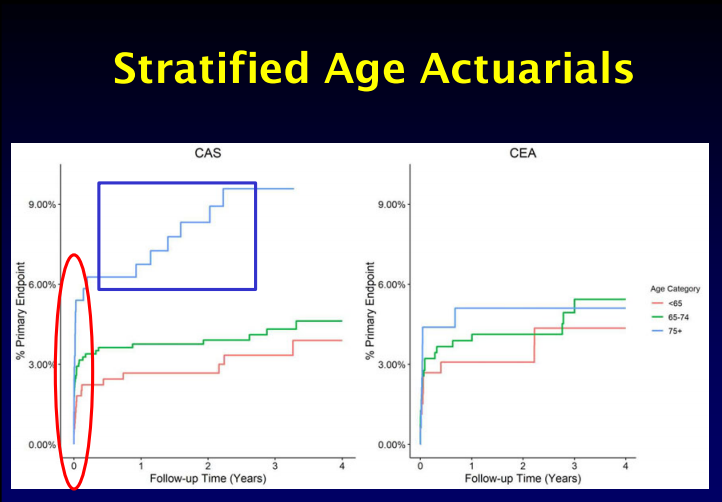
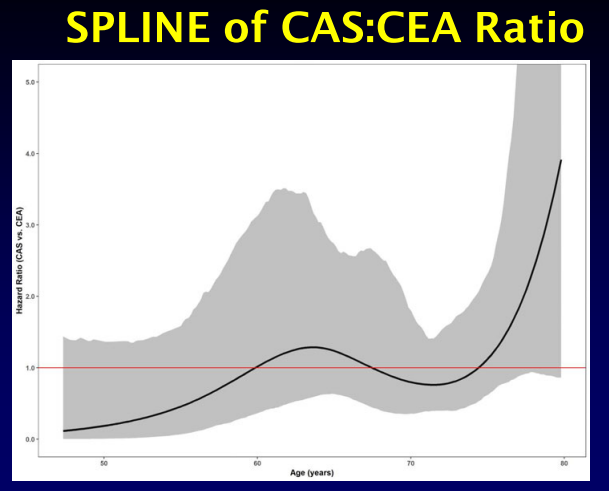
Figure 2. analysis of risk differences in age subgroups
Sex subgroups: in the CAS group, the pooled incidence of perioperative death, stroke, or myocardial infarction was similar in women and men. In the CEA group, the primary outcomes were also similar between genders. Further comparison of the pooled outcomes of death and stroke further minimized the gender differences between the CAS and CEA groups (Figure 3).
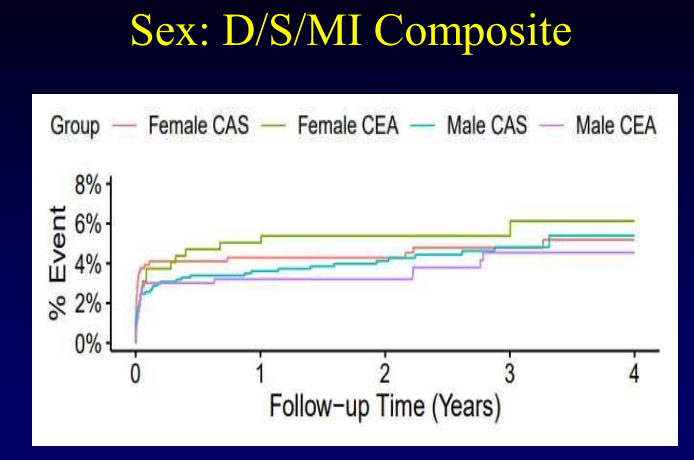
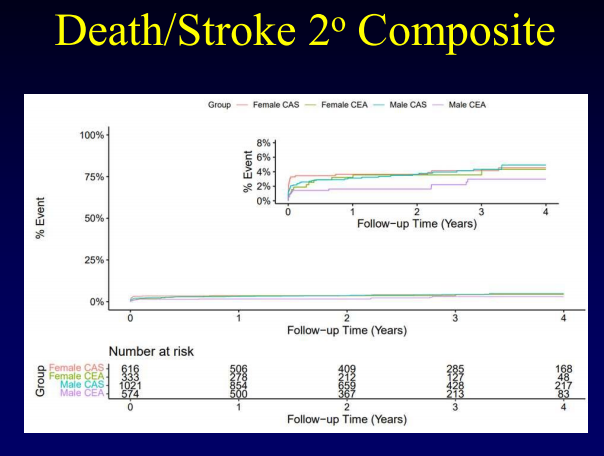
Figure 3.Analysis of risk differences in gender subgroups
summarize
In a pooled analysis of randomized standard-risk, asymptomatic patients <80 years of age with carotid stenosis, there was no statistically significant difference in the incidence of postoperative complications and 4-year ipsilateral stroke between CAS and CEA. Based on the age-stratified analysis, the incidence of postoperative death/stroke was significantly higher with CAS than with CEA in the older age group (75-79 yr); therefore, CAS is not suitable for older, asymptomatic patients. Based on the gender analysis, it was shown that there was no significant difference between females and males in terms of the primary outcomes after both CAS and CEA.
Reprinted from Outpatient
