

Peripheral arterial disease (PAD) is the leading cause of lower extremity amputations and a major risk factor for cardiovascular death. As more attention is paid to PAD and the number of studies grows, more researchers are focusing on patients from minority populations.In 2012, the American Heart Association (AHA) called for addressing gender-related disparities in PAD, pointing to the need for increased clinical awareness, focused treatment plans, and expanded research efforts. Despite recent findings suggesting an increased prevalence of PAD in women, PAD in women remains underdiagnosed and understudied. At the 50th International Vascular and Endoluminal Vascular Congress (VEITH 2023), November 14-18, US local time, Professor Linda M. Harris from the Jacobs School of Medicine and Biomedical Sciences at the University at Buffalo, USA, shared gender differences in the clinical presentation of lower extremity occlusive disease and intermittent claudication and the importance of this phenomenon.

The insidious nature of women's PAD problems
With the increased emphasis on PAD and the growing number of studies, more attention is being paid to women with PAD, who have long been underappreciated in the past. Previous PAD studies have focused on male patients, and recent studies have found similar or higher prevalence of PAD in women and men. Women have a 2-fold increase in the prevalence of CLTI, multisegmental lesions are more common, women with PAD are less likely to be claudicant compared with men (again according to the criterion of an ABI of<0.9), and="" the="" prevalence="" of="" pad="" is="" higher="" in="" nonsmokers="" than="" men="">
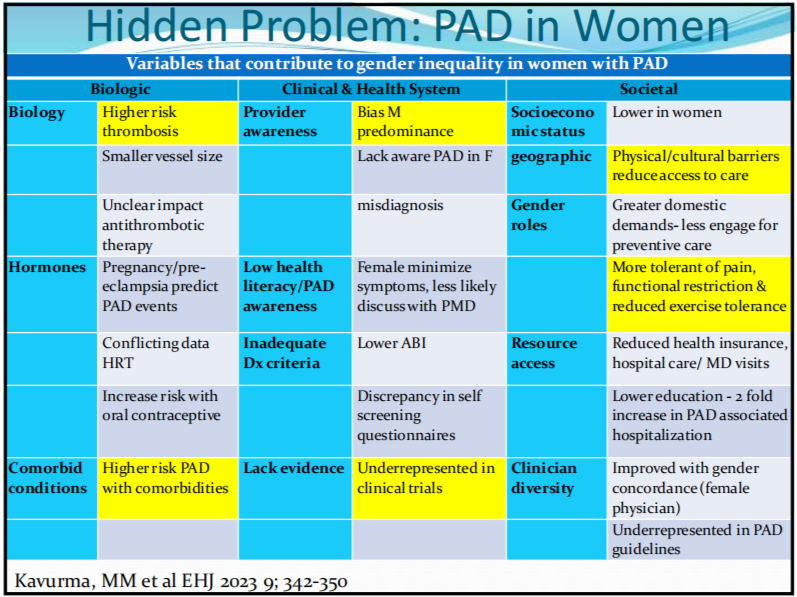
Table 1: Variables contributing to gender differences in PAD
Gender differences in risk factors for PAD
(1) Smoking: Men are more likely to have a history of smoking, but smoking affects women more. Former smokers have a 3-fold increased risk of developing PAD, and current smokers have a 10-fold increased risk of developing PAD.
(2) Diabetes: Women with impaired glucose tolerance have a higher risk of developing PAD.
(3) Hyperlipidemia: women with PAD have a higher prevalence of hyperlipidemia.
(4) Nontraditional risk factors: female patients may also be at risk for hypertensive disorders of pregnancy and autoimmune disorders (i.e., RA, which is more common in females.) Women with CKD<70 50="" have="" a="">
(5) Biomarkers: triacylglycerol, hsCRP, and GGT are associated with PAD in women (metabolic, inflammatory); fibrinogen, NT-pro-BNP, and 25-OH vitamin D are more highly correlated with PAD in men (coagulopathy).
Gender differences in the typicality of PAD symptoms
There were differences in symptom presentation between male and female PAD patients: male PAD patients tended to be in the claudication stage, while female PAD patients were either asymptomatic or had developed CLTI; symptom presentation was more typical for males and atypical for females; and the proportion of medical treatment/attendance: 67% of male PAD patients had medical treatment, compared with 19% of females (P = 0.011; Table 2).
Only 10% of ALL patients have typical symptoms, 50% have atypical symptoms, and 40% are asymptomatic, with asymptomatic symptoms being more prevalent in women. The following atypical symptoms have been defined in the WHAS (Women's Health and Aging) study: slowed gait, fatigue, numbness of the limbs, difficulty with stairs, difficulty with walking 1/4 mile, difficulty in balancing and stability, pain with exertion that is not relieved by rest, pain with exertion that does not result in discontinuation of movement, pain that begins at rest, pain that is not relieved by rest, pain that does not result in discontinuation of movement, pain that begins at rest. pain on exertion that is not relieved by rest, pain on exertion that does not result in discontinuation of movement, and pain that begins in the resting state. Atypical symptoms were missed both because patients did not report symptoms themselves (self-limited walking, slow gait) and because patients reported symptoms but did not take them seriously.
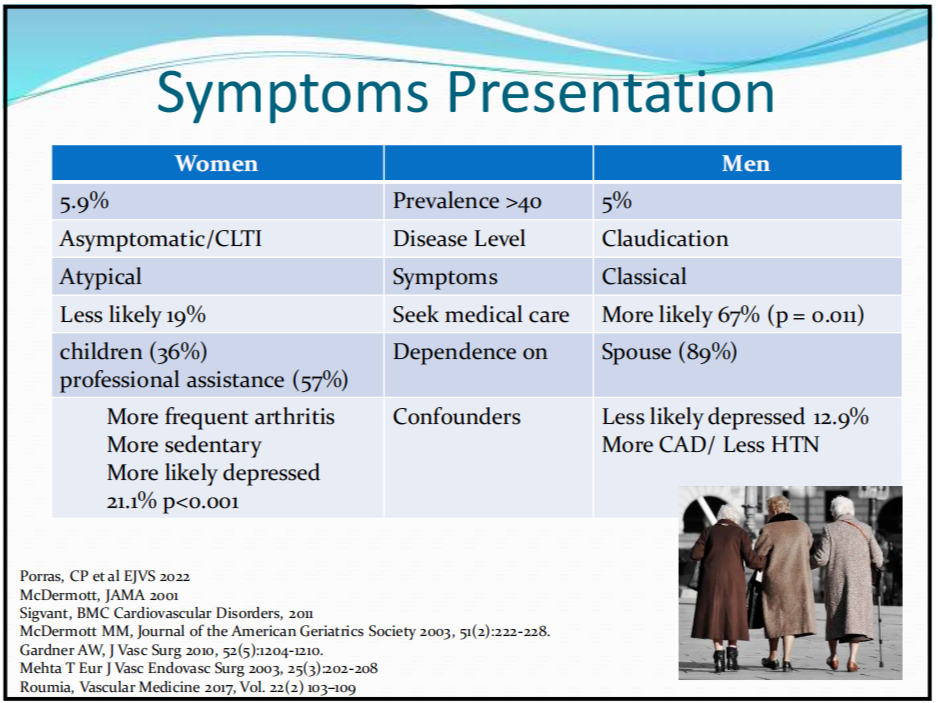
Table 2. gender differences in PAD symptom presentation
Differences in the impact of gender on functional impairment
Functional impairment due to PAD tended to be more severe in women, as evidenced by a 33% reduction in time to claudication onset, a 23% reduction in maximum walking distance, slower walking speed (shorter 6-minute walking distances), a greater reduction in walking ability, and poorer quality of life scores. Painful symptoms reported in the data related to male PAD patients were more pronounced, whereas functional impairment was more severe in female PAD patients.
Summary
Female PAD patients tend to have more atypical symptoms, in addition to the fact that they are more often missed or diagnosed later due to socioeconomic reasons, biological reasons (comorbidities, hormone levels, and other effects), and clinical reasons (physician awareness/data). Delay in diagnosis can lead to suboptimal and inadequate patient outcomes, delayed timing of treatment, progression of CLTI, and worsening quality of life levels. New studies on peripheral arterial disease should evaluate male and female patients separately and should actively recruit female subjects.
转载至《门诊》杂志
