
Presenter: Michel Bosiers, MD
Hospital: Department of Vascular Surgery, University Hospital Bern, Switzerland
Abstract: Shockwave L6 IVL catheter enables minimally invasive revascularization for complex iliac calcified occlusion, avoiding open surgery.
Introduction
Calcified iliac artery occlusion presents significant therapeutic challenges. Conventional angioplasty risks underexpansion and rupture. Prof. Bosiers' team innovatively applied the Shockwave L6 IVL catheter to achieve safe revascularization in a high-risk case.
Case Study
1.Patient Profile:
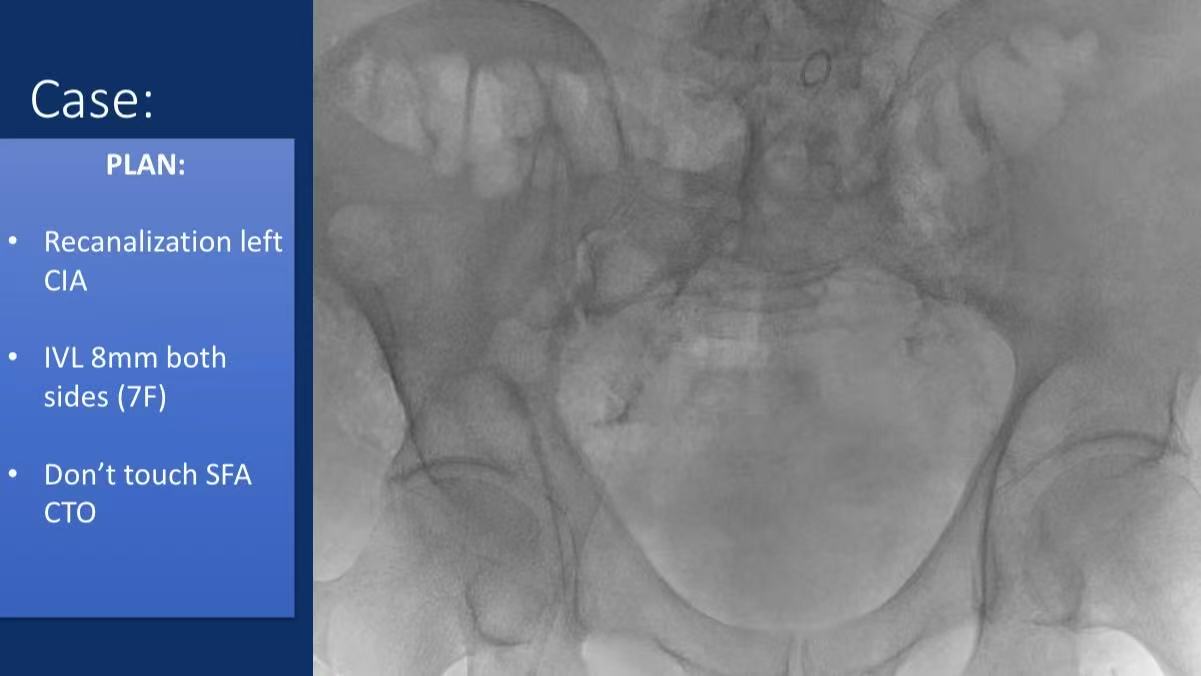
Lesion: Left common iliac artery (CIA) occlusion
Key Decision: Preserved left SFA CTO to avoid multilevel intervention risks
Goal: Unilateral iliac revascularization
2.IVL L6 Procedure:
Device: Bilateral 8mm balloons (7F-compatible)
Calcium Modification:
Sonic pressure waves at 2-4atm
Targeted fracture of deep calcium (>180° arc)
Adjunctive: 10×38mm BeSmooth balloon post-dilation

3.Outcomes
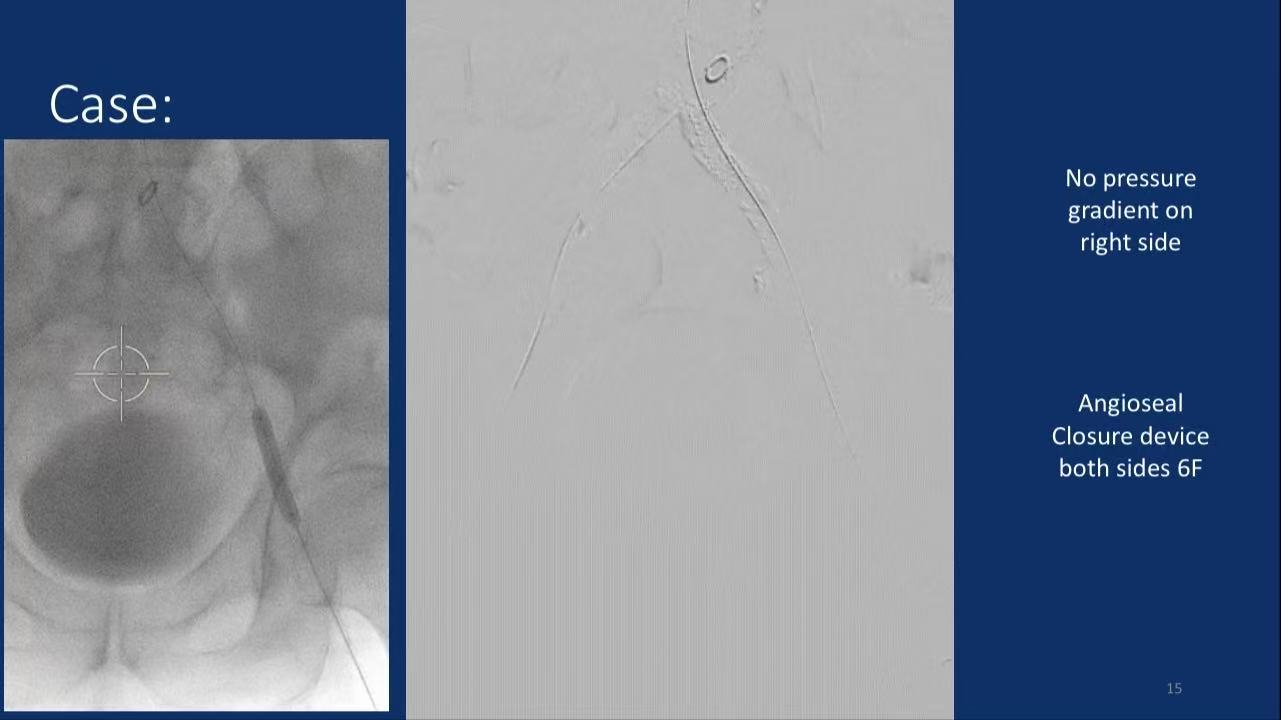
Pressure Gradient: Absent on right side
Closure: Bilateral 6F AngioSeal (no complications)
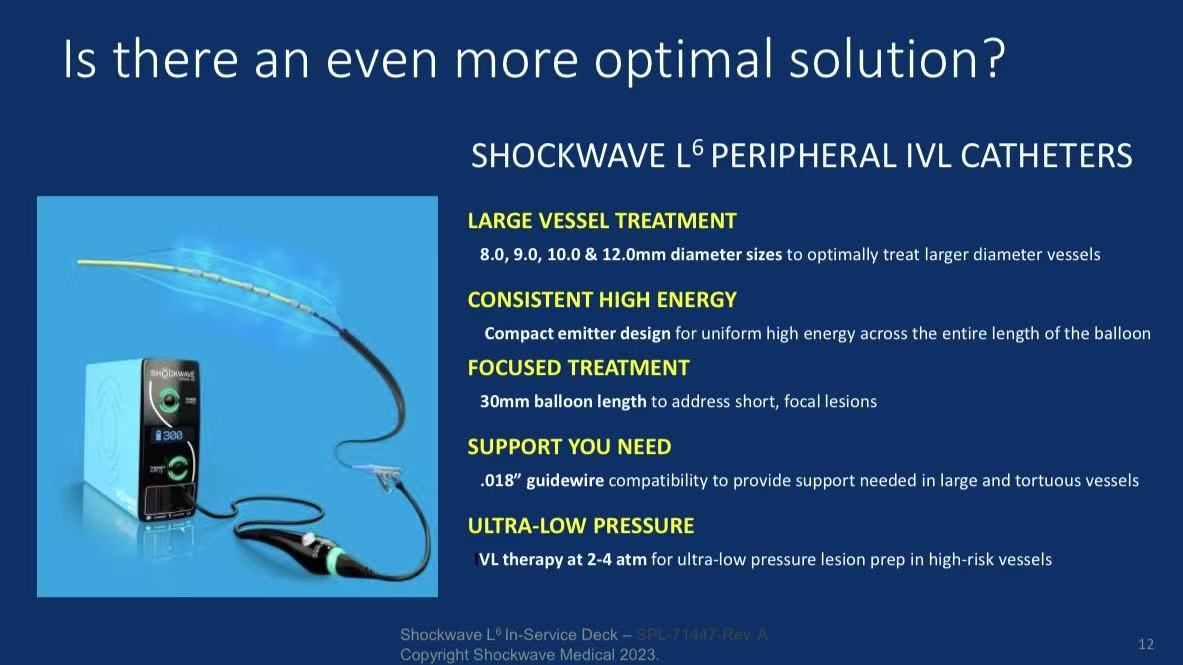
Technology Highlights:
Large-Vessel Compatibility:
8-12mm diameters cover iliac/CFA (>20% US peripheral interventions)
30mm balloon for focal calcification
Safety Innovations:
0.018" guidewire compatibility enhances trackability (successful CIA crossing)
Selective calcium modification (acoustic waves target calcified tissue only, density differential >80x)
Clinical Efficiency:
Single-device therapy (vs. rotational/laser atherectomy)
40% reduction in procedure time
Conclusions
1.Paradigm Shift:
IVL L6 avoids open surgery in 80% of aortoiliac calcified cases
Ideal for high-risk anatomy (e.g., bifurcation, internal iliac preservation zones)
2.Future Directions:
TAVR/EVAR access preparation (per Frank Arko)
Long-term patency validation (ongoing follow-up)
