Presenter: Celso Nunes
Hospital: Vascular Surgery Department, Coimbra, Portugal
Abstract
A 71-year-old female with coral reef aorta and bilateral limb ischemia underwent descending thoracic aorta (DTA)-to-femoral/iliac bypass. Postoperatively, claudication resolved, and pedal pulses were restored. This approach avoids hostile abdominal conditions and reduces visceral ischemia risk.
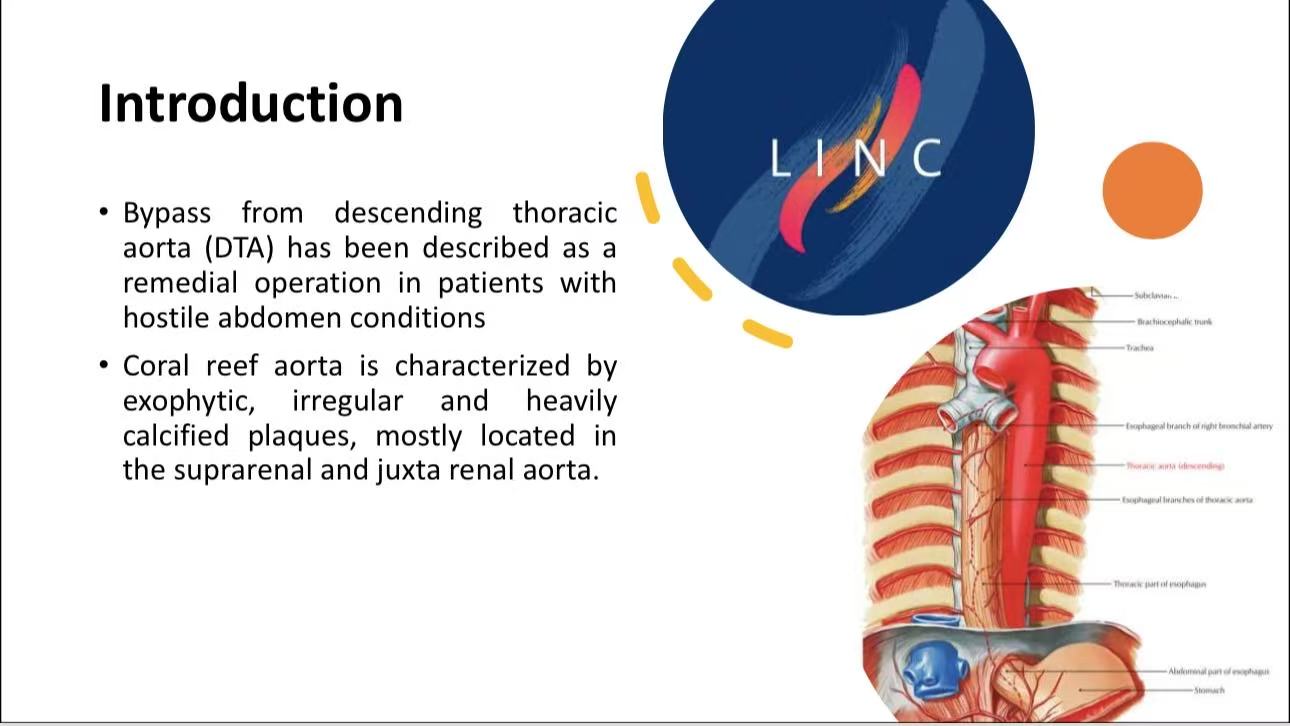
Introduction
Coral reef aorta often precludes standard aortic clamping. DTA bypass provides alternative inflow, particularly in patients with extensive calcification or prior abdominal surgeries.
Case Analysis
Patient Profile: Incapacitating claudication (20–30 meters), absent femoral pulses.
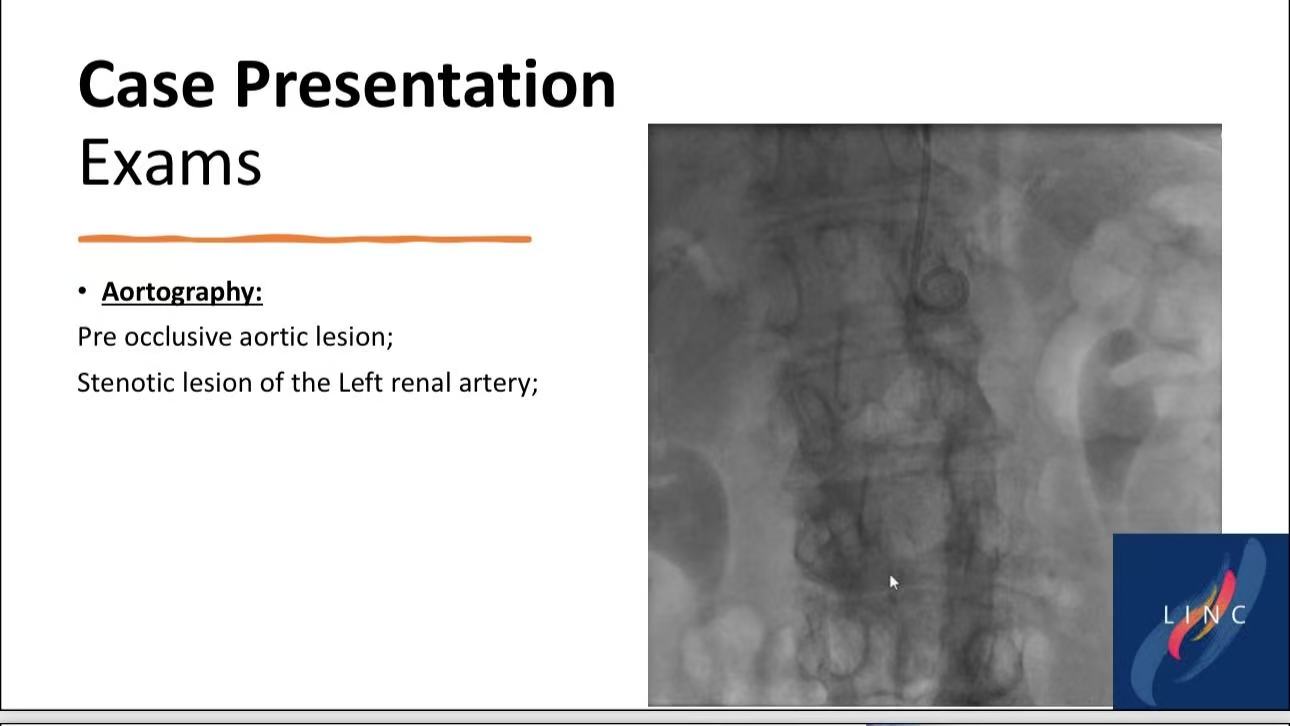
Imaging: Pre-occlusive aortic stenosis, left renal artery involvement.

Surgical Steps:
Right semi-lateral decubitus with posterolateral thoracotomy.

DTA-to-femoral/iliac anastomosis using bifurcated Dacron graft.

Outcome: Discharge at 10 days; symptom-free at 1 year.


Technical Considerations
Graft Tunneling: Anterior to left kidney to avoid kinking.
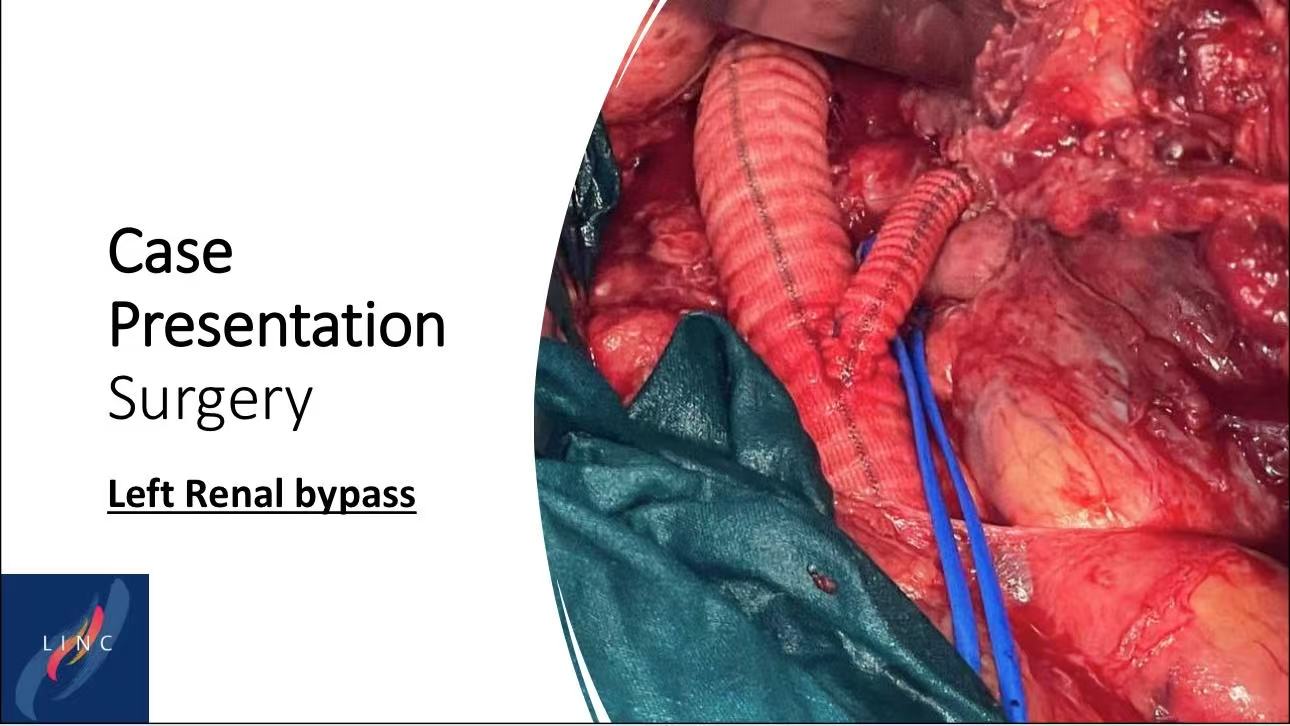
Renal Protection: Partial aortic clamping preserved renal perfusion.
Conclusion
1.DTA bypass is a durable solution for coral reef aorta with low perioperative morbidity.
2.Recommendation: Reserve for patients with prohibitive abdominal pathology.