Presenter: Peter B. Anderson
Hospital: Mayo Clinic, Rochester, USA
Abstract
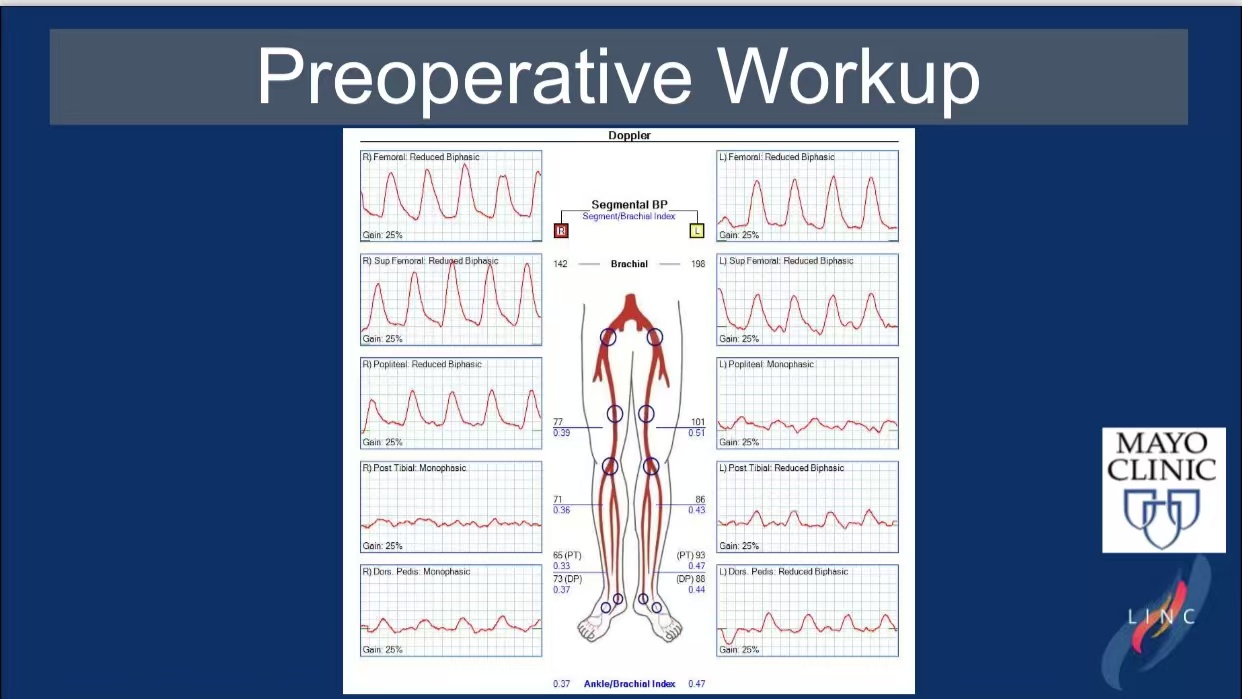
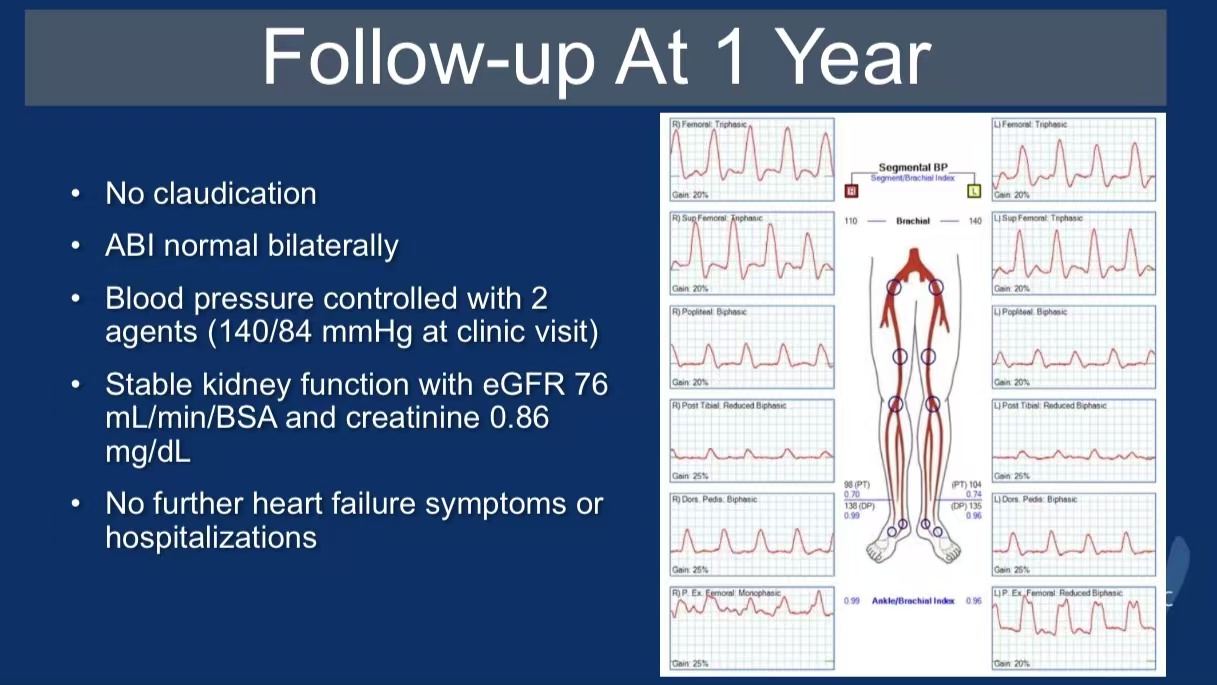
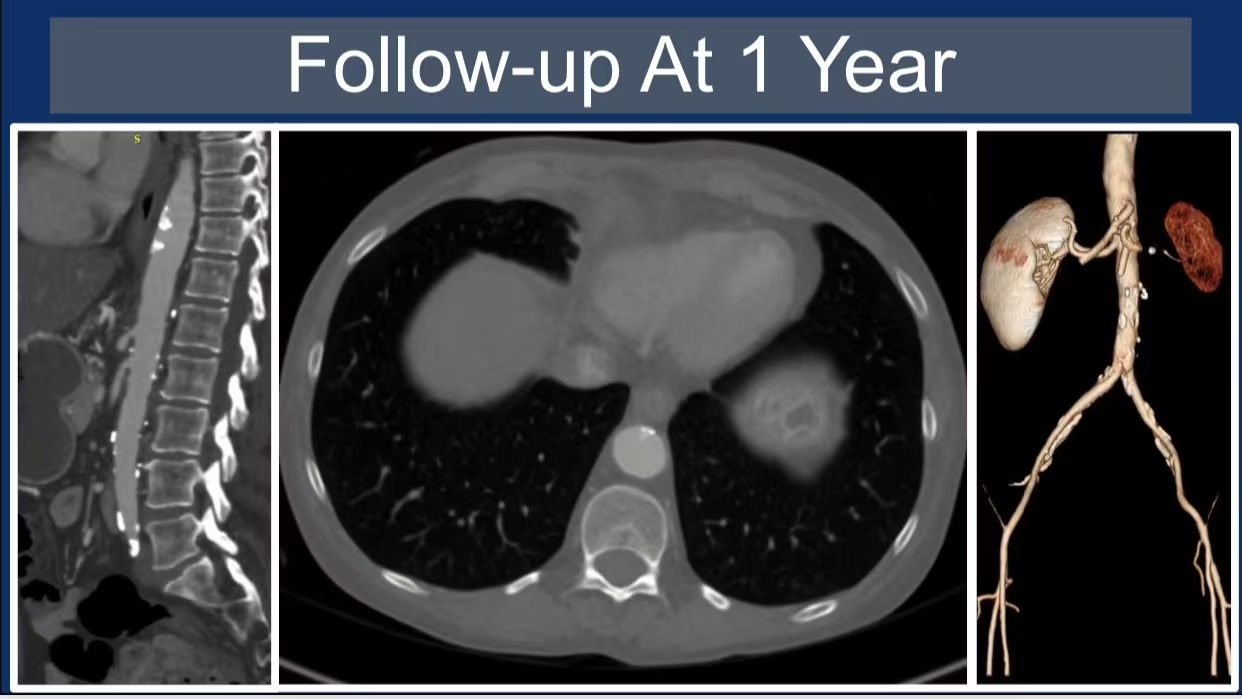
A 56-year-old female with paravisceral coral reef plaque underwent transaortic endarterectomy, resolving claudication and renovascular hypertension. Postoperative ABI normalized (0.37→1.0), and 1-year follow-up confirmed sustained patency. This case highlights the efficacy of open surgical intervention in complex aortic calcification.
Introduction
Coral reef aorta, characterized by calcified exophytic plaques, often requires aggressive intervention due to mesenteric ischemia and renovascular complications. Transaortic endarterectomy offers direct plaque removal while preserving aortic integrity.
Case Analysis
Clinical Profile: Severe bilateral claudication, uncontrolled hypertension (SBP >200 mmHg), and CKD.
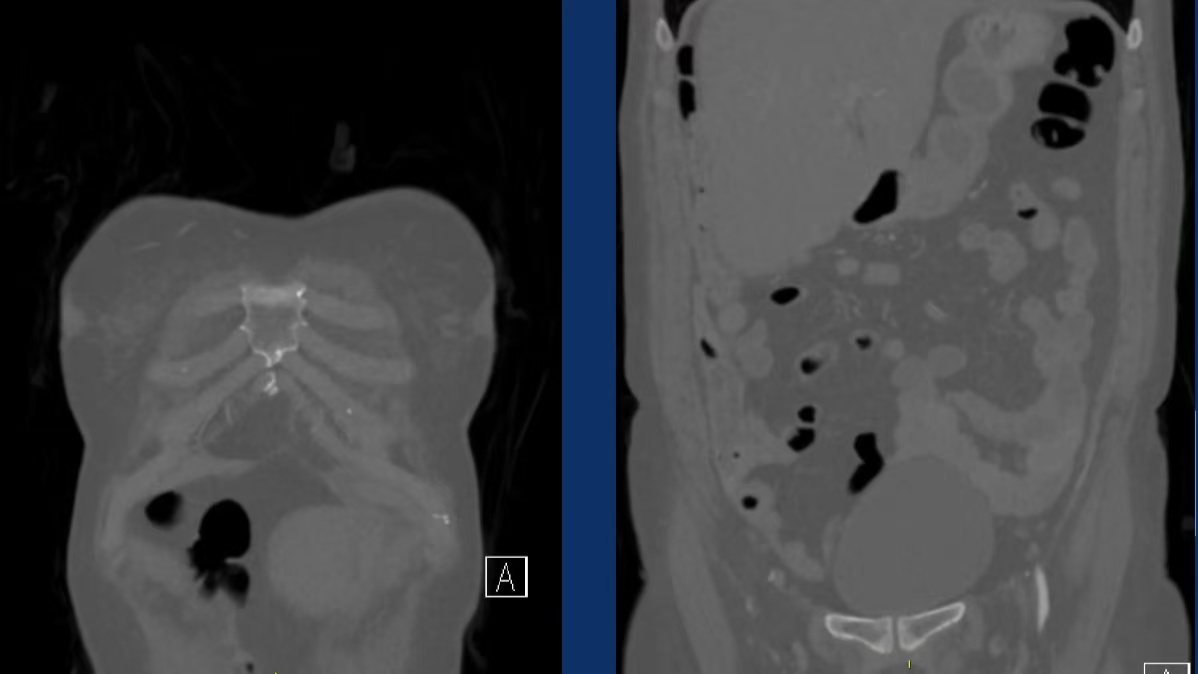
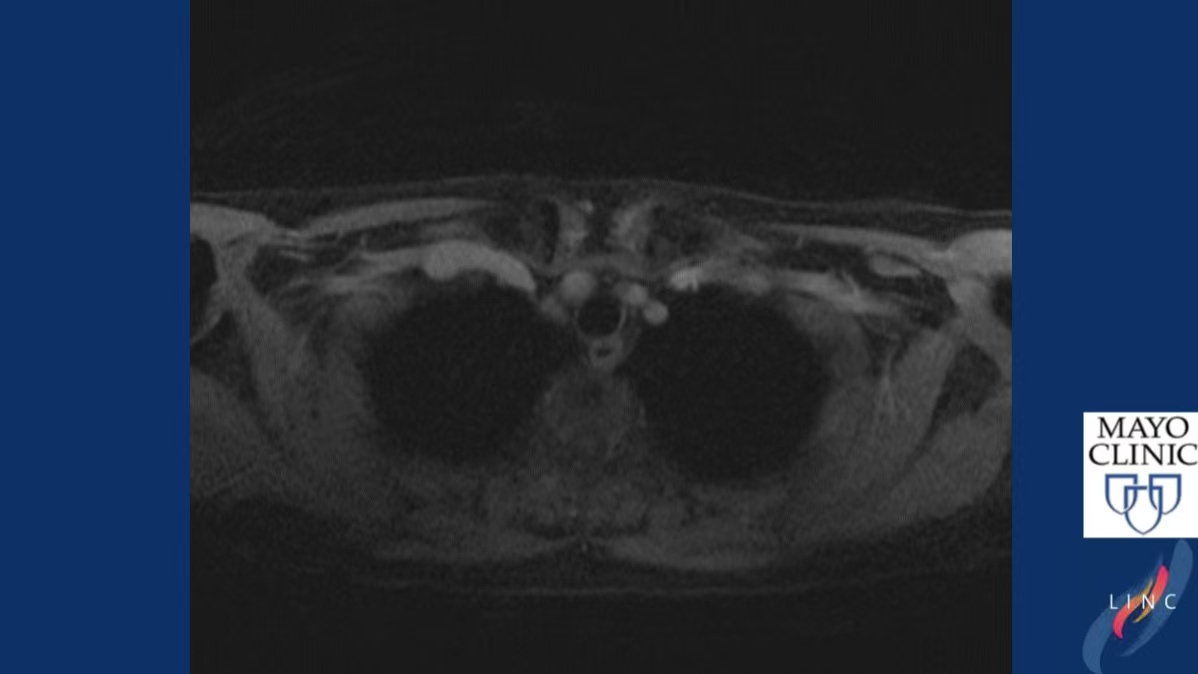
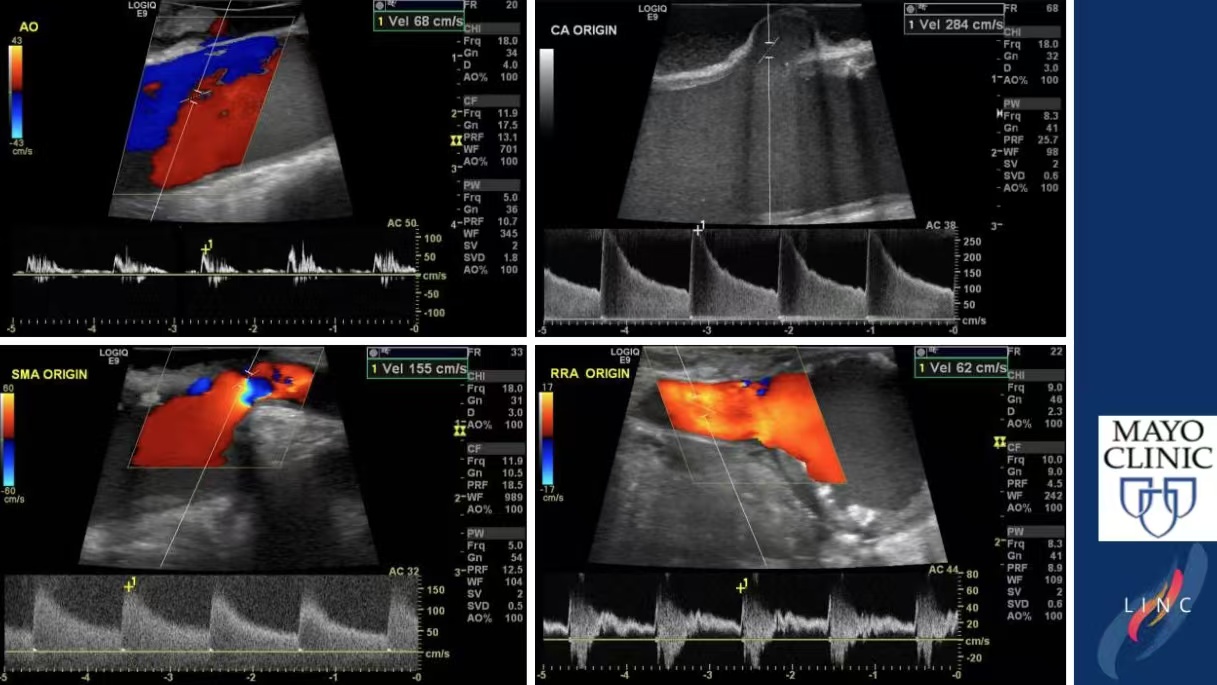
Imaging: Coral reef plaque involving visceral aortic branches.


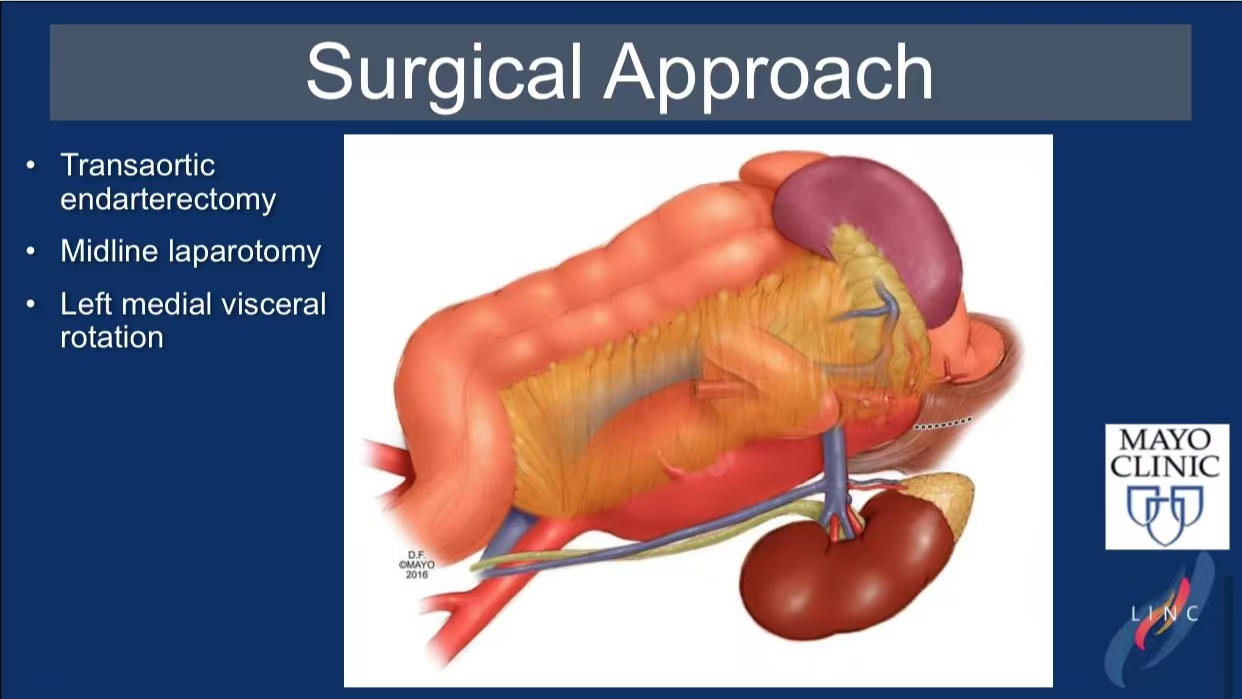
Surgical Technique:
•Midline laparotomy with left medial visceral rotation.
•Transaortic endarterectomy under partial clamping.
Outcome: Immediate symptom resolution; eGFR improved from 71 to 76 mL/min/BSA.
Discussion
Advantages: Avoids prosthetic grafts; reduces risk of spinal cord ischemia.
Challenges: Requires meticulous dissection to prevent arterial perforation.
Conclusion
1.Transaortic endarterectomy is optimal for young patients with localized disease.
2.Practice Tip: Prioritize partial clamping to minimize ischemic time.