
The "2022 Asian Endovascular Training Course (ATC)" was successfully held on November 22, 2022, Beijing time, sponsored by the National Center for Cardiovascular Diseases, undertaken by Fuwai Hospital Affiliated to the Chinese Academy of Sciences, with the China Vascular Congress as the academic support unit and the Hi Heart Voice Project Team as the media support unit.
The Asian Endovascular Training Course (ATC) program brings together many influential experts and scholars in Asia, with the purpose of "collaboration, communication, and improvement", in line with the principles of more scientific, authoritative, objective and practical, to convey the cutting-edge progress of cardiac surgery, inspire new ideas to overcome cardiac surgical diseases, provide a high-level platform for academic exchanges and learning, better assist clinicians in endovascular diagnosis and treatment, and provide strong support for clinical decision-making.
At the meeting, Professor Sanghyun Ahn from the Department of Vascular Surgery, Seoul National University Hospital, South Korea, gave a wonderful speech on "Preparation of Endovascular Plan".
EVAR is not superior to other procedures in terms of outcomes in patients with poor neck anatomy or normal AAA.
Endovascular abdominal aortic aneurysm repair (EVAR) is inseparable from a variety of devices, and the main products currently used in Korea are: Medtronic Endurant II./II.s, Cook zenith, Cordis Incraft, SnG Biotech*seal, Medtronic Helix-Fx, Cook IBD, etc., each of which has its own advantages and disadvantages. The number of patients with abdominal aortic aneurysm (AAA) undergoing EVAR surgery in Korea is increasing year by year, and is now three times the number of patients undergoing open surgical repair (OSR). In clinical practice, there has been a high prevalence of EVAR outside of the Specific Instruction for Use (IFU).
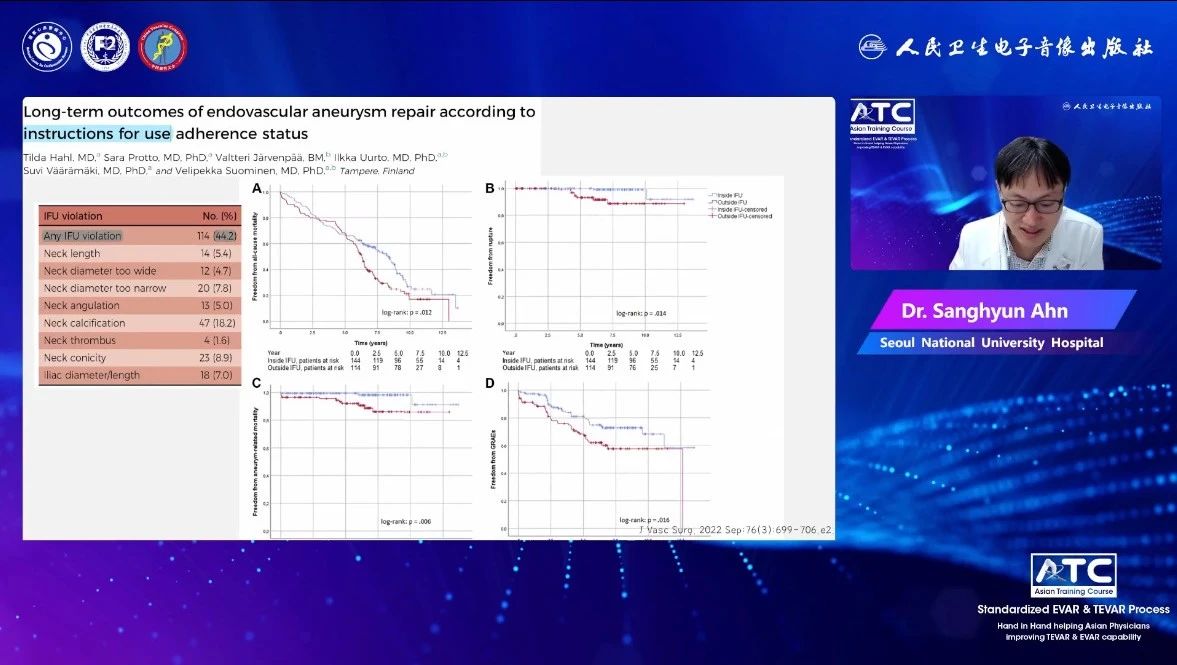
A study in Finland showed that about 44.2% of physicians did not fully adhere to the product's IFU when performing EVAR surgery. EVAR outside of IFU had a significant effect on all-cause mortality (HR 1.39; 95% CI 1.02-1.89; P = 0.37) and AAA-related mortality (HR 5.1; 95% CI 1.4-18.6; P = 0.15), as well as AAA rupture (HR 5.4; 95% CI 1.1-26.6; P = 0.36).
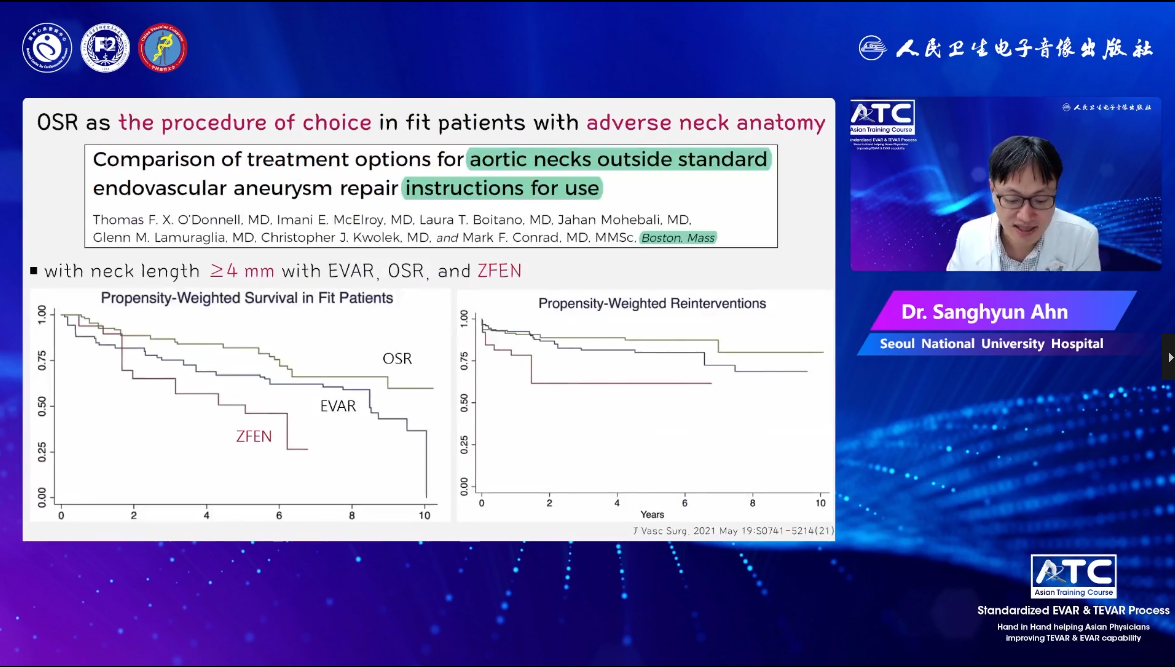
Imani E McElroy et al. also demonstrated in their study that EVAR procedures performed outside the IFU were associated with a higher incidence of type IA endoleak (22% at five years, 2% within the IFU, HR 5.8; 95% CI 3.1-10.9, P). <0.01) and lower survival (5- and 10-year survival: 56% and 34% vs 81% and 53%, HR: 2.3 95% CI 1.2-4.3, P = 0.01). For patients who are not within the scope of the EVAR IFU, OSR is associated with higher long-term survival. OSR should be superior to EVAR or commercially available fenestration stent systems (ZFEN) in appropriate patients.
EVAR has been uneven in terms of satisfaction with the treatment of patients with poor tumor neck anatomy or normal AAA. In this regard, the UK recommends the use of OSR, while countries such as Europe recommend EVAR. The choice of procedure should be judged based on multiple aspects, including the patient's experience, medical costs, and the merits of the product. There are many reasons why EVAR is performed outside of IFU, mainly in terms of aortic aneurysm neck length and aneurysm neck angle. Currently, Seoul National University Hospital (SNUH) divides the aortic aneurysm neck into four types: A, B, C, and D according to the length and angle of the neck. Type A has a length > 10mm and an angle ≤ 60°, type B has a length > 10mm and an angle of > 60°, type C has a length of <10mm and an angle of ≤ 60°, and type D has a length of < 10mm and an angle of > 60°, of which type A and type B account for more, 73.7% and 21.2% respectively.
A study in Japan has confirmed that the Push-Up technology combined with the Endurant stent transplantation system can be safely and effectively used in the treatment of patients with severe distorted tumor neck.
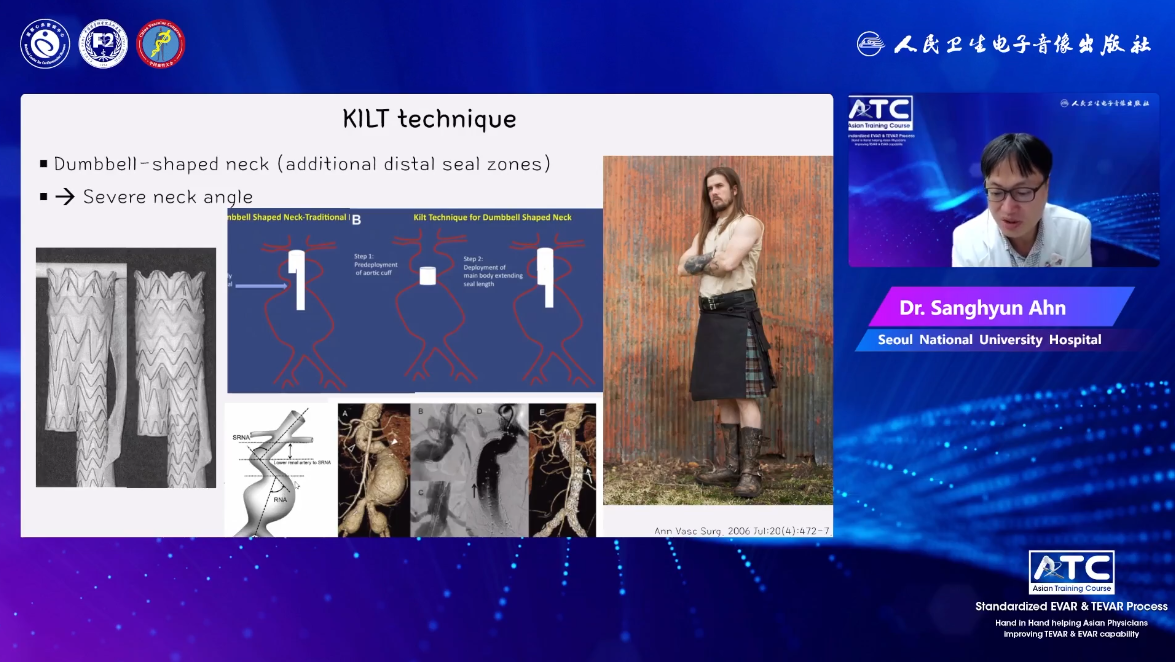
KILT (Kilt) technology for AAAs with dumbbell-shaped necks or severely angulated necks in confined areas distally.
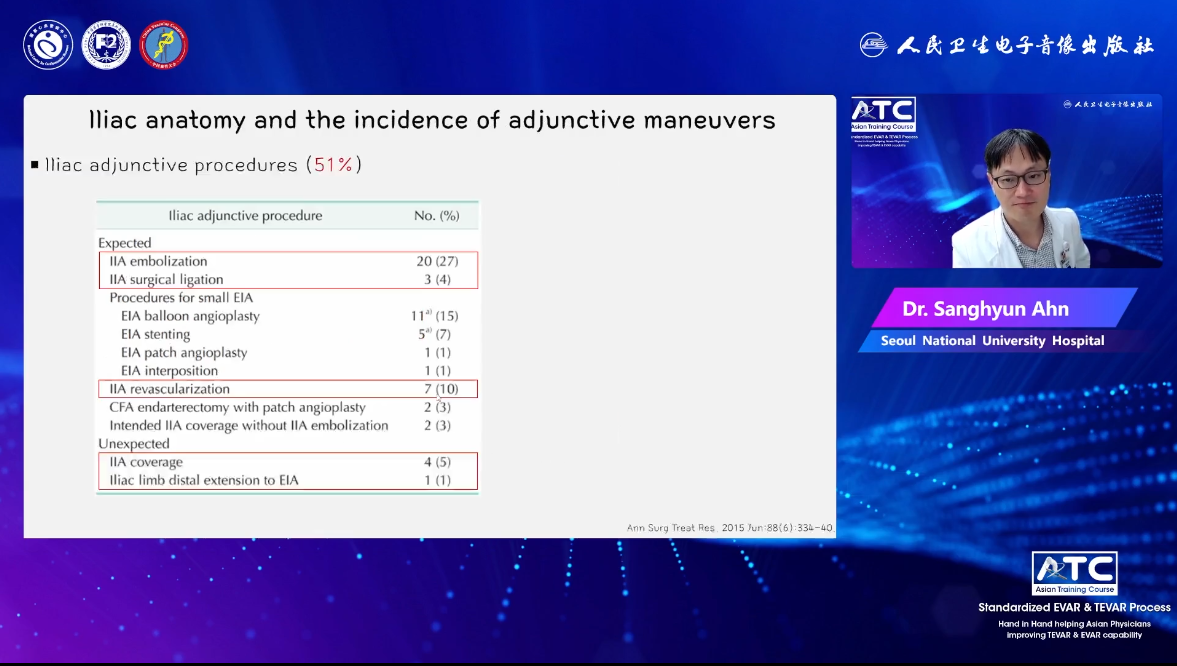
When the assistive device is applied to the challenging EVAR, due to the physiological and anatomical differences between the Eastern and Western human bodies, such as the length of the common iliac artery (CIA) in Asians is shorter than that in Westerners, many patients have related difficulties in accessing, but most of them are overcome by endovascular or hybrid techniques, and the use of assistive devices is conducive to the smooth progress of EVAR.
What we should note is:
1. Abdominal aortic aneurysm assist devices are part of the "endovascular preparation plan", but these auxiliary devices are still in the experimental stage, and their short- and long-term results are uncertain.
2. OSR or EVAR should be comprehensively considered according to the patient's acceptance of surgery-related complications, awareness of lifelong imaging examinations, and socio-economic burden.
3. In medical centers with large sample sizes, OSR is still a reasonable choice for the treatment of poor neck anatomy or normal abdominal aortic aneurysm.
