
The "2022 Asian Endovascular Training Course (ATC)" was successfully held on November 22, 2022, Beijing time, sponsored by the National Center for Cardiovascular Diseases, undertaken by Fuwai Hospital Affiliated to the Chinese Academy of Sciences, with the China Vascular Congress as the academic support unit and the Hi Heart Voice Project Team as the media support unit.
The Asian Endovascular Training Course (ATC) program brings together many influential experts and scholars in Asia, with the purpose of "collaboration, communication, and improvement", in line with the principles of more scientific, authoritative, objective and practical, to convey the cutting-edge progress of cardiac surgery, inspire new ideas to overcome cardiac surgical diseases, provide a high-level platform for academic exchanges and learning, better assist clinicians in endovascular diagnosis and treatment, and provide strong support for clinical decision-making.
At the meeting, Professor Luo Mingyao from Fuwai Hospital, Chinese Academy of Medical Sciences, gave a wonderful speech on "Chinese Expert Consensus and Experience of Hybridization Technology in Arch Aortic Lesions".
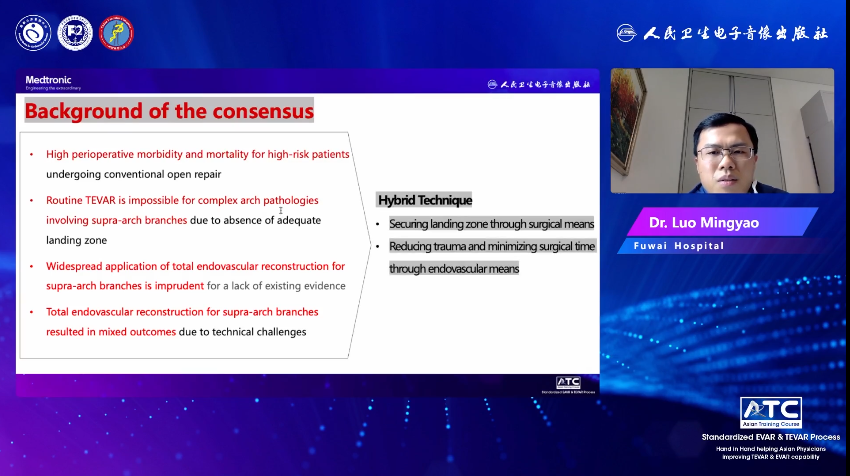
Background to the formation of expert consensus on hybridization technology
According to the relevant data of patients treated by Fuwai Medical of the Chinese Academy of Medical Sciences in recent years, the anatomical location of aortic lesions is mainly dominated by the aortic root and arch, and with the progress of national aging, the number of patients over 60 years old is also increasing year by year, and accounting for a large proportion. Due to the complexity of anatomical location and the particularity of variant deformity, it is difficult to correct aortic arch disease, and some complex lesions cannot be treated with conventional TEVAR due to the lack of sufficient anchoring area. Therefore, our team proposed the "HENDO" technology system that combines hybrid technique (H), endovascular repair (Endo) and open surgery (O) to treat aortic arch lesions, so as to improve the survival rate and quality of life of patients. This technique minimizes trauma and shortens the duration of surgery through a combination of surgical and endoluminal methods.
An introduction to hybridization techniques
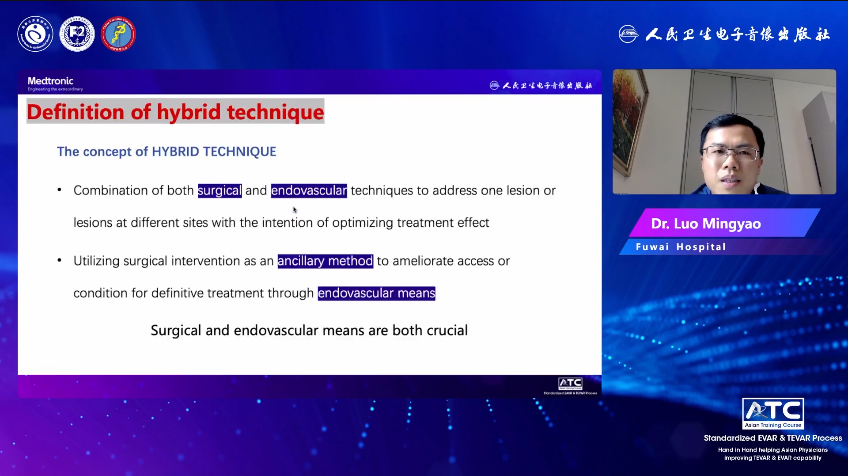
● The concept of hybridization technology
Hybridization technology mainly includes the following two aspects:
1.The combination of surgery and endovascular intervention, using different measures to treat the lesions or treating the lesions in different parts respectively, and the two apply their own strengths to achieve the best effect;
2. Surgical means are used as auxiliary measures to create convenient and feasible paths or conditions for endovascular operation, and finally directly repair or isolate the lesions and treat the disease through endovascular technology and equipment. Surgery and endovascular interventions are both critical and mutually reinforcing.
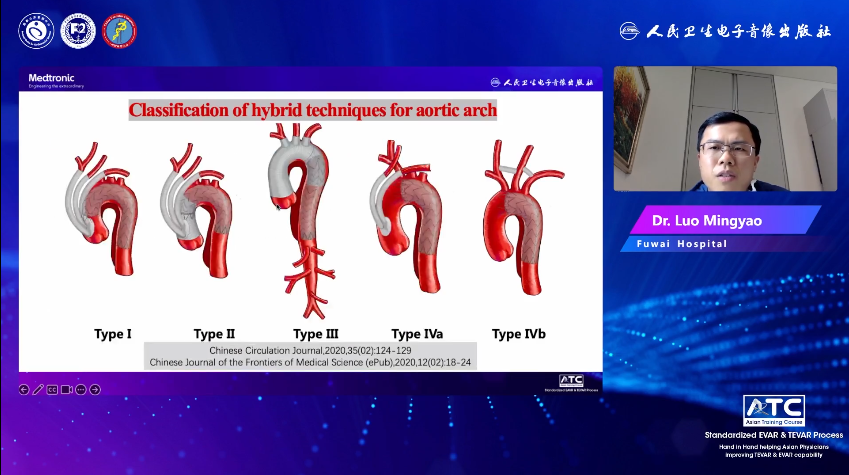
● Typing of hybridization techniques
There are 4 types of hybrid techniques for the treatment of aortic arch diseases. The first 3 types are hybrid total aortic arch repairs, and the IV types are partial aortic arch repairs. According to the relevant data of patients admitted to Fuwai Hospital from 2017 to 2020, the most commonly used classification is Hybrid II., accounting for about 76%.
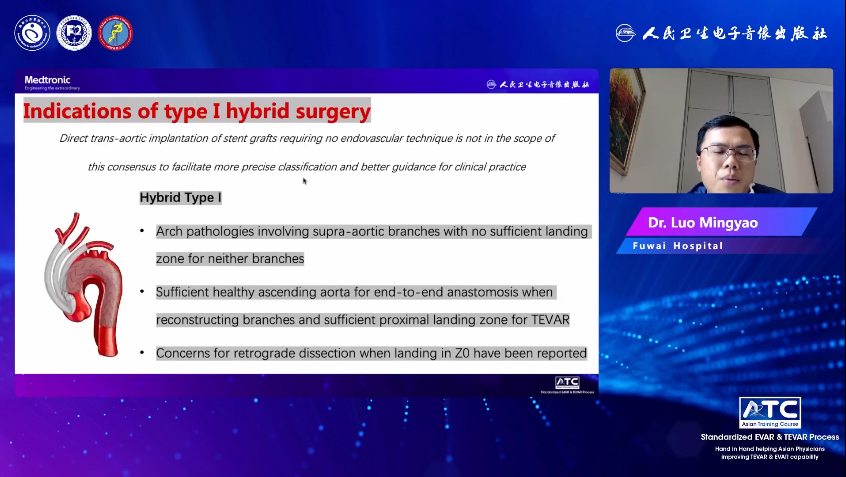
1. Hybrid type I is a non-cardiopulmonary bypass descending ascending aorta-supraarch vascular bypass, combined with endovascular repair of aortic total arch stent graft, and the stent graft is anchored in the Z0 area of the ascending aorta;
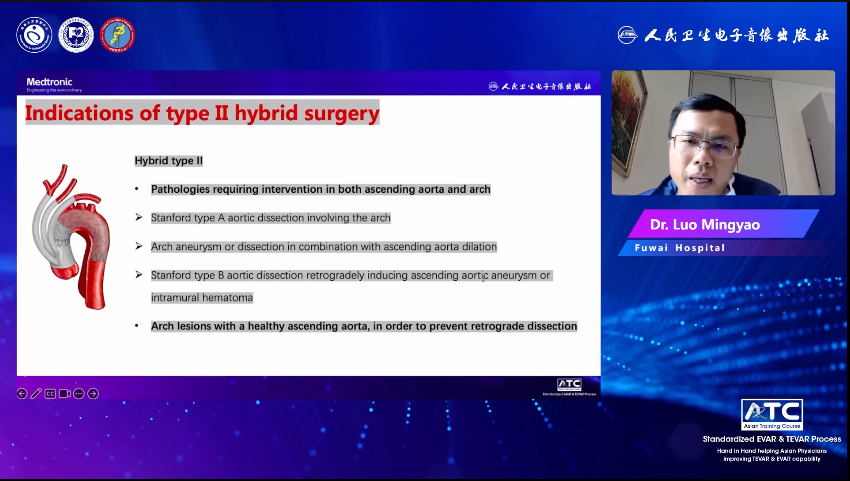
2. Hybrid II is the ascending aortic replacement (with or without treatment of the aortic root) and the de-branching of the superior arch artery under cardiopulmonary bypass, combined with endovascular repair of the aortic total arch stent graft, and the stent graft is anchored to the artificial blood vessel;
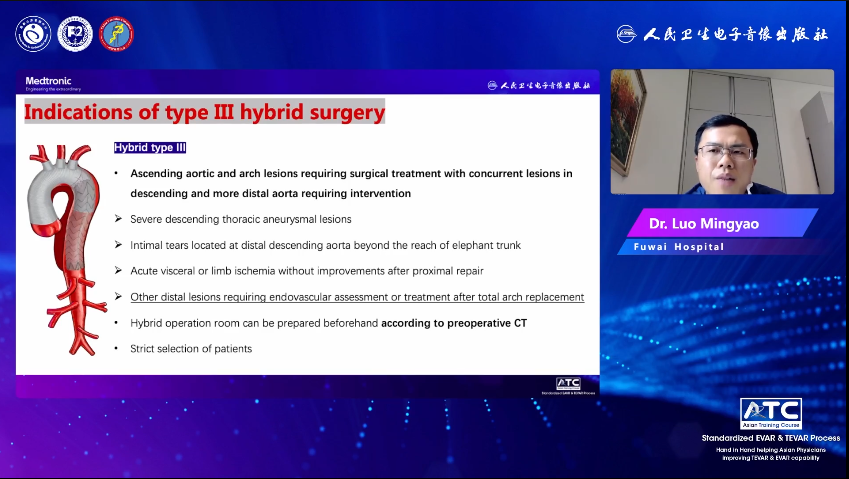
3. Hybrid Type III. is the replacement of the ascending aorta (with or without treatment of the aortic root) and the aortic arch under the cryogenic arrest of circulation, and the elephant trunk stent can be placed, and then the descending aorta and distal lesions that cannot be treated by conventional open surgery can be evaluated or repaired with the help of guidewire catheter technology;
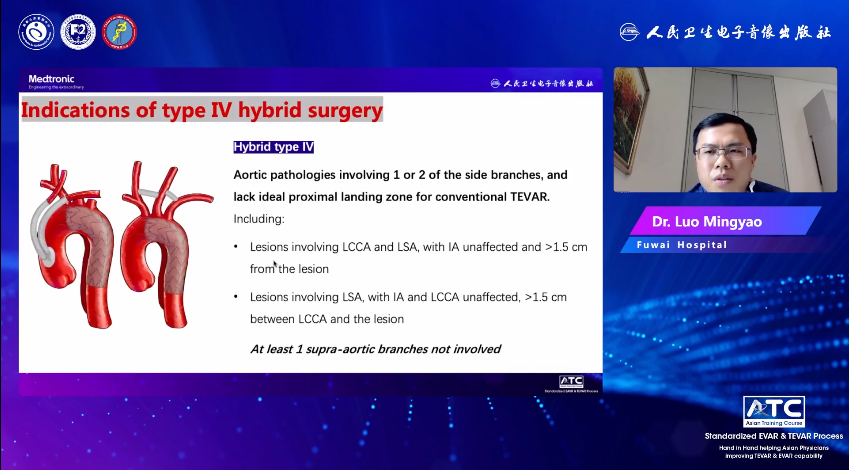
4. Hybrid type IV is partial aortic arch repair. It is characterized by the stent graft covering part of the branch opening of the aortic arch, that is, under the non-cardiopulmonary bypass, one or two artificial vascular diversion of the ascending aorta-arch artery (type IV.a) is performed under thoracotomy, or the artificial vascular diversion of the neck vessel is performed without thoracotomy (type IV.b), combined with endovascular repair of part of the aortic arch stent graft. In hybrid surgery, the implantation of stent graft is mostly retrograde implantation through the femoral artery in the conventional way, and in special cases, it can also be implanted through the thoracic prosthetic vascular perfusion branch.
Indications for hybridization techniques
1. Hybrid Type I Aortic Arch Repair: The aortic arch lesion involves the supraarch branch artery, and there is no sufficient anchoring distance from each branch, and there is no obvious lesion in the ascending aorta, which can provide enough safe area for reconstruction of the aortic side anastomosis of the supraarch branch and provide sufficient stent anchoring area. In addition, it is worth noting that there are reports that there is a certain risk of back-tearing when the Z0 zone is used as the stent anchoring area.
2. Hybrid type II aortic arch repair: Ascending aorta and arch lesions require surgical treatment, and the descending aorta is not significantly dilated. For example, Stanford type A aortic dissection involves the arch, and the aortic arch aneurysm or dissection combined with ascending aorta dilation; The tear is located in the arch or at the beginning of the descending aorta, but the dissection is retrograde to the ascending aorta or aortic dissection with significant intermural hematoma in the ascending aorta. Some patients with a normal ascending aorta may also be included to avoid the risk of reverse tears. This procedure is preferentially recommended for patients over 60 years of age. For young patients with many comorbidities, poor general condition, and high risk of cryogenic cycle arrest surgery, Hybrid II surgery can also be considered after strict screening and discussion.
3. Hybrid III. Aortic Arch Repair: Ascending aorta and arch lesions require surgical treatment, and those with descending aortic lesions and more distant aortic lesions require interventional treatment. If accompanied by descending thoracic aortic aneurysm-like changes, total arch surgery alone cannot completely resolve the lesion; or the larger breach is located in the middle and distal segment of the descending aorta, and the length of the trunk stent cannot be reached; or acute ischemia of distal organs and limbs, and there is no improvement after surgery; Other patients who require the guidewire catheter technique to evaluate and manage distant lesions after total arch replacement.
4. Hybrid IV. partial aortic arch repair: the aortic lesion involves part of the arch branch vessels, and the conventional thoracic endovascular aortic repair lacks an ideal anchoring area, including two conditions: (1) the lesion involves the left common carotid artery opening and the left subclavian artery, but is not involved at a >distance of 1.5cm from the distal end of the innominate artery opening; (2) The lesion involved the left subclavian artery, but was not involved at > 1.5 cm distal to the left common carotid artery opening.
summary
1.This is the first expert consensus on the treatment of aortic arch lesions by hybridization technology in China;
2. This consensus summarizes common hybrid techniques, which not only facilitates international exchanges, but also reflects Chinese characteristics;
3. In the future, as the evidence increases, we expect to see hybridization techniques gradually standardized to further improve the quality of life of patients.
