
The "2022 Asian Endovascular Training Course (ATC)" was successfully held on November 22, 2022, Beijing time, sponsored by the National Center for Cardiovascular Diseases, undertaken by Fuwai Hospital Affiliated to the Chinese Academy of Sciences, with the China Vascular Congress as the academic support unit and the Hi Heart Voice Project Team as the media support unit.
The Asian Endovascular Training Course (ATC) program brings together many influential experts and scholars in Asia, with the purpose of "collaboration, communication, and improvement", in line with the principles of more scientific, authoritative, objective and practical, to convey the cutting-edge progress of cardiac surgery, inspire new ideas to overcome cardiac surgical diseases, provide a high-level platform for academic exchanges and learning, better assist clinicians in endovascular diagnosis and treatment, and provide strong support for clinical decision-making.
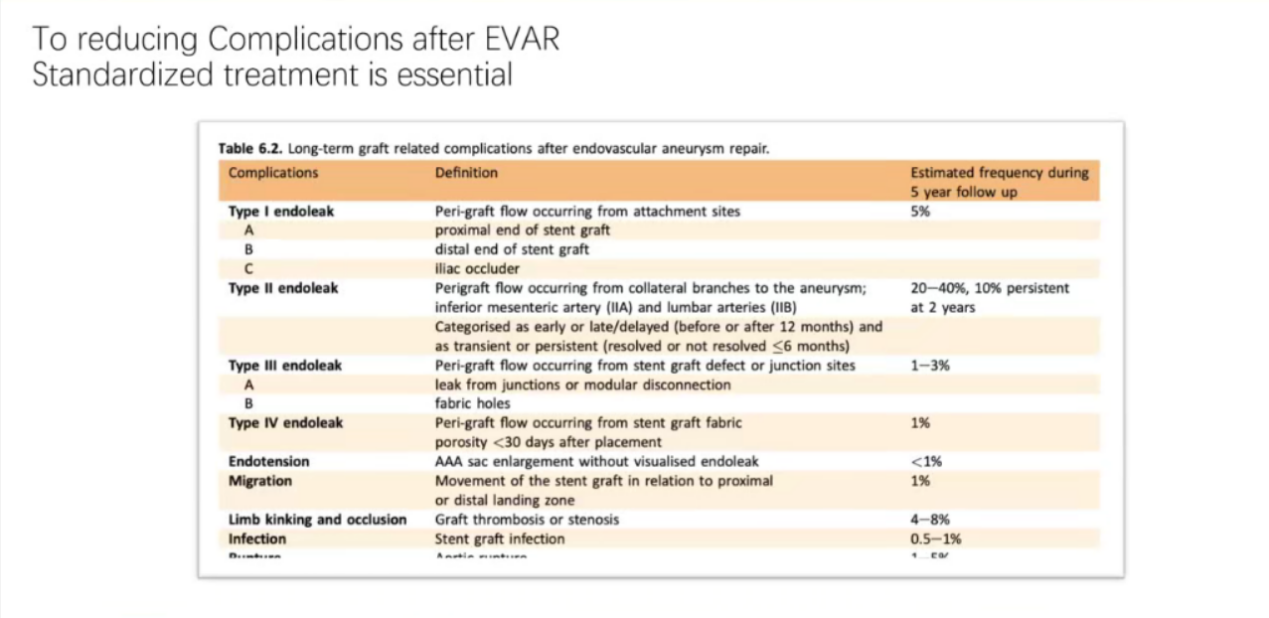
Standardized treatment for endovascular aortic surgery is essential. The number of aortic surgeries in China has increased year by year, the number of endovascular surgeries and open surgeries has increased, and the number of endovascular repair surgeries has increased rapidly, and there are significant differences in the postoperative outcomes of endovascular repair surgeries in different provinces in China. Among them, complications after endovascular aortic repair include endoleak (endoleak occurs around the graft, 10% of type II endoleak during the follow-up period occurs 2 years after surgery), internal tension (aurculum dilation in the absence of obvious endoleakage), stent displacement, stent twisting and occlusion, infection (stent graft infection), rupture (aortic rupture), etc.
As a national vascular disease center, Fuwai Hospital admits a large number of patients who undergo reoperation after endovascular therapy, and the second operation is especially difficult due to the existence of such complications, so we emphasize the importance of standardized treatment of endovascular aortic surgery.
With the widespread use of EVAR, safety and efficacy are paramount. Based on the guidelines, consensus and clinical experience of vascular surgeons in Fuwai Hospital, the surgical process of Fuwai was introduced by taking endovascular repair of abdominal aortic aneurysm as an example. It aims to improve the success rate of surgery, reduce complications, shorten operation time, reduce fluoroscopy time and contrast agent consumption, and benefit both doctors and patients. Standardized treatment of endovascular aortic surgery is essential to reduce the complications of EVAR (endovascular repair of abdominal aortic aneurysm), including preoperative evaluation and planning, including careful selection of patients (meeting surgical indications, no anatomical contraindications, no treatment contraindications), pathological evaluation (pathological features, anatomy, aortic wall condition, approach, anchoring area, measurement method), and surgical algorithm planning (repair strategy, technique, stent type, stent size).
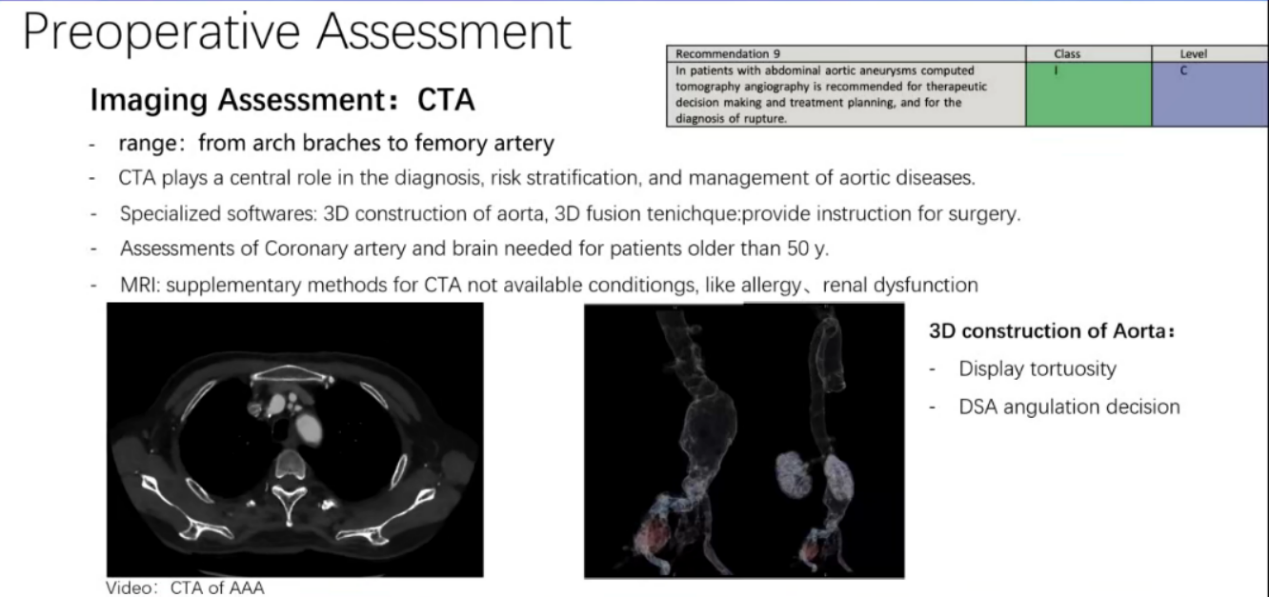
CTA plays an important role in the diagnosis, risk stratification and treatment of aortic disease, and can be used to provide guidance for surgery using 3D modeling and 3D fusion technology of aorta. MRI may be used as an adjunct in cases where CTA is contraindicated, such as contrast allergy and renal insufficiency.
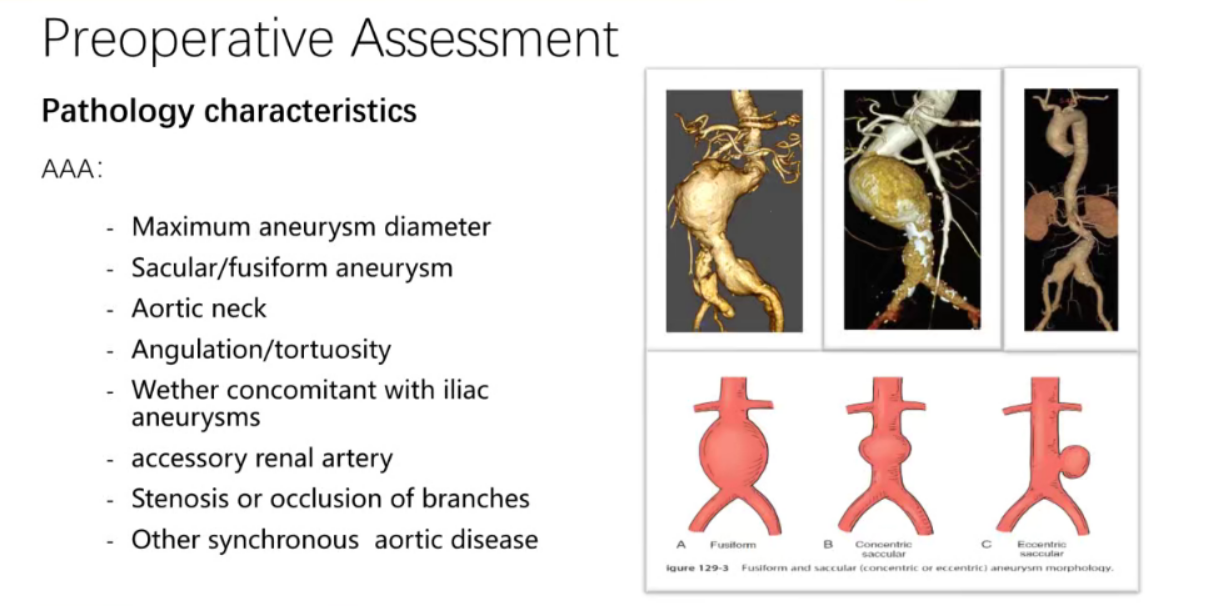
Abdominal aortic aneurysms should be evaluated preoperatively for pathologic features, including maximum aneurysm diameter, fusiform or cystic aneurysm, aortic aneurysm neck, aneurysm angle/curvature, presence of accessory renal arteries with iliac artery aneurysm, stenosis or occlusion of branch arteries, and other concomitant aortic lesions. In terms of surgical approach, the femoral artery is the most common access option, and the vascular diameter of the femoral artery approach is >7mm, and the conventional delivery sheath is usually selected, and the < 7mm is usually selected, and the Minis stent system can be selected.
Relative contraindications to the vascular approach approach include severe inguinal trauma, high femoral artery bifurcation, need for frequent catheter sheath replacement, significant proximal iliac occlusive disease, smaller diameter iliofemoral artery, severe calcification of the femoral artery.
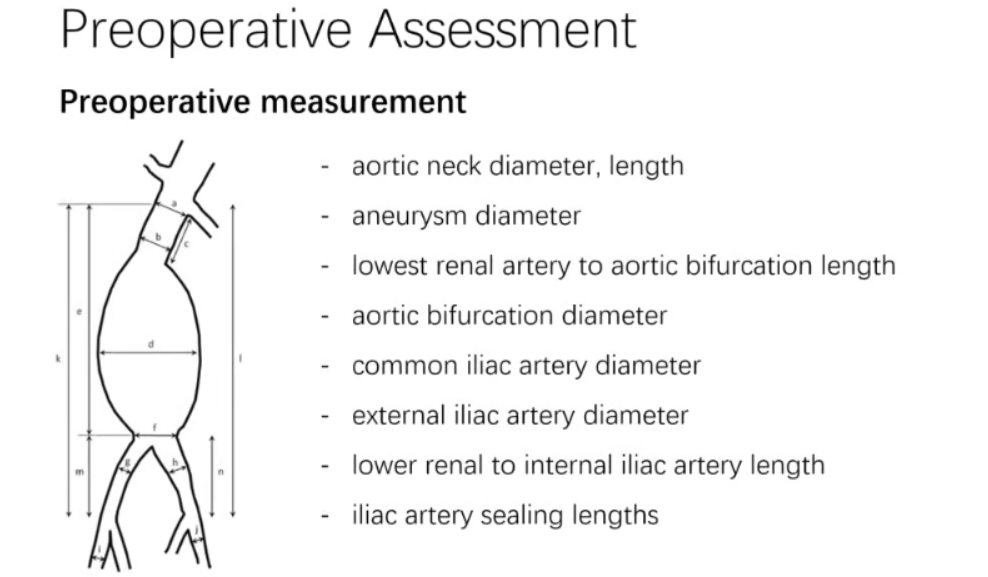
Both the proximal and distal anchored areas need to be assessed for a normal aorta of sufficient length. The 2014 ESC guidelines recommend that the proximal anchoring area of EVAR should be 10-15 mm and the diameter should be < 32 mm, and the risk of stent displacement and endoleakage is significantly increased when the neck twist angle is greater than 60 degrees. For most brackets, an anchor area of 2-2.5cm is more suitable. In general, the longer the anchoring area, the lower the risk of endoleak and displacement, and in the case of aneurysms, longer anchoring areas are better able to cope with long-term degenerative changes. The data that need to be measured before surgery include aortic aneurysm neck diameter, length, aneurysm diameter, minimum renal artery to aortic bifurcation length, aortic bifurcation diameter, common iliac artery diameter, external iliac artery diameter, minimum renal artery to internal iliac artery length, iliac artery coverage length, etc.
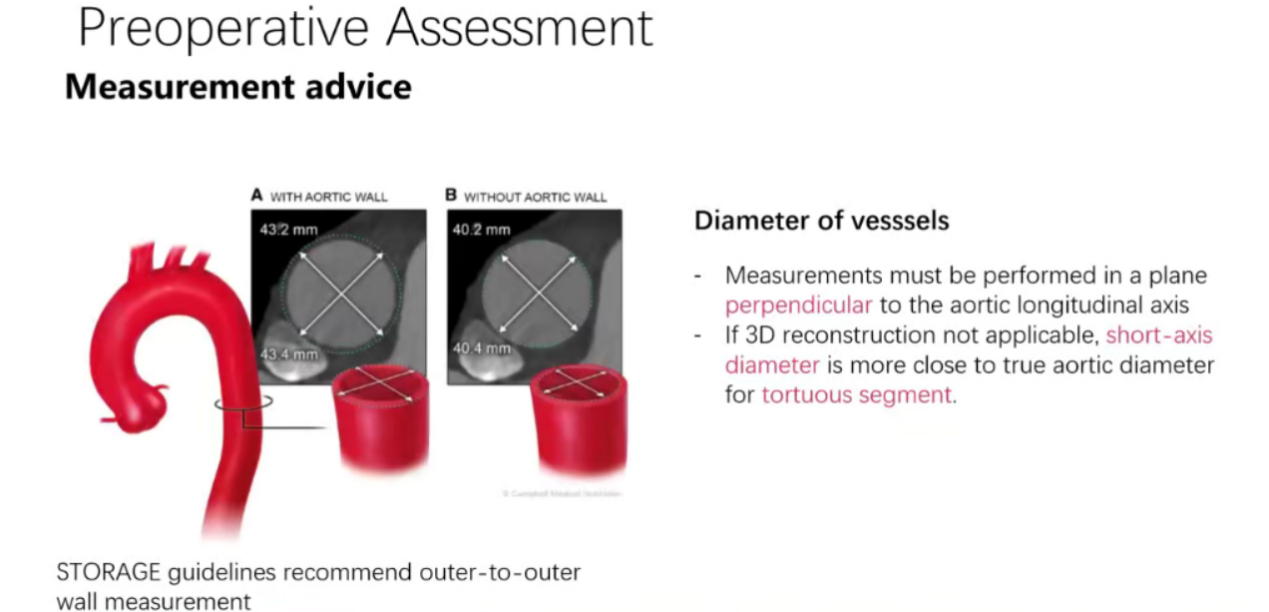
For the assessment of vessel diameter, the STORAGE guidelines recommend that the measurement of the outer wall of the artery to the outer wall should be performed in a plane perpendicular to the longitudinal axis of the aorta, and if 3D reconstruction is not applicable, the diameter of the short axis is closer to the tortuous segment of the true diameter of the aorta. At the same time, EVAR technology also includes fenestration/parallel stenting/custom stent technology for abdominal aortic aneurysm in the proximal renal artery, as well as iliac artery reconstruction technology. The size of the stent includes the diameter and length, and the magnification of 10-20% is recommended for the diameter, and it is necessary to pay attention to the situation that the magnification is too large and will cause the stent to fold.
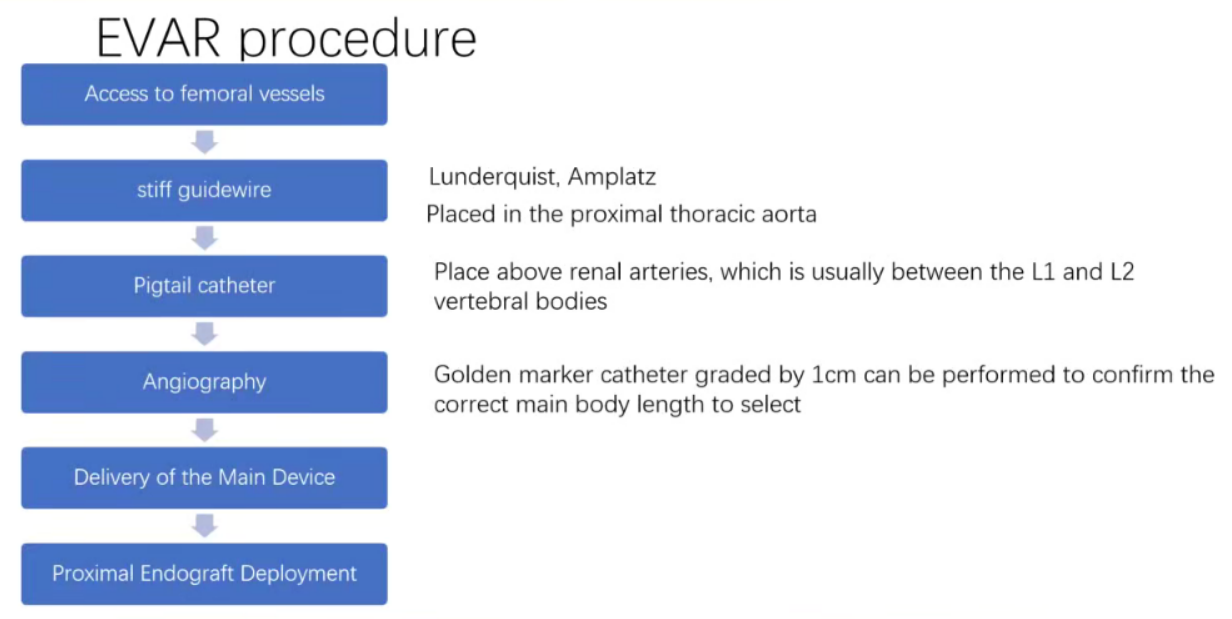
The EVAR (endovascular repair of abdominal aortic aneurysm) procedure involves access to the femoral artery, a rigid guidewire placed proximal to the thoracic aorta, and a pigtail catheter placed above the renal artery, usually between the L1 and L2 vertebrae, followed by angiography, introduction of the stent body device, and release of the proximal end of the main stent. Conventional preoperative and postoperative angiography is performed once each, and after the first angiogram, the relative angle of the C-arm to the patient remains the same, and the stent is positioned and released by bony markers and preoperative angiography, thereby reducing the contrast dose and radiation time. After the stent is released, the balloon kiss technique is emphasized to dilate the abdominal aorta and bilateral iliac artery stents throughout the whole process, so that the stent graft can be fully dilated, and the stent compression and thrombosis are reduced.
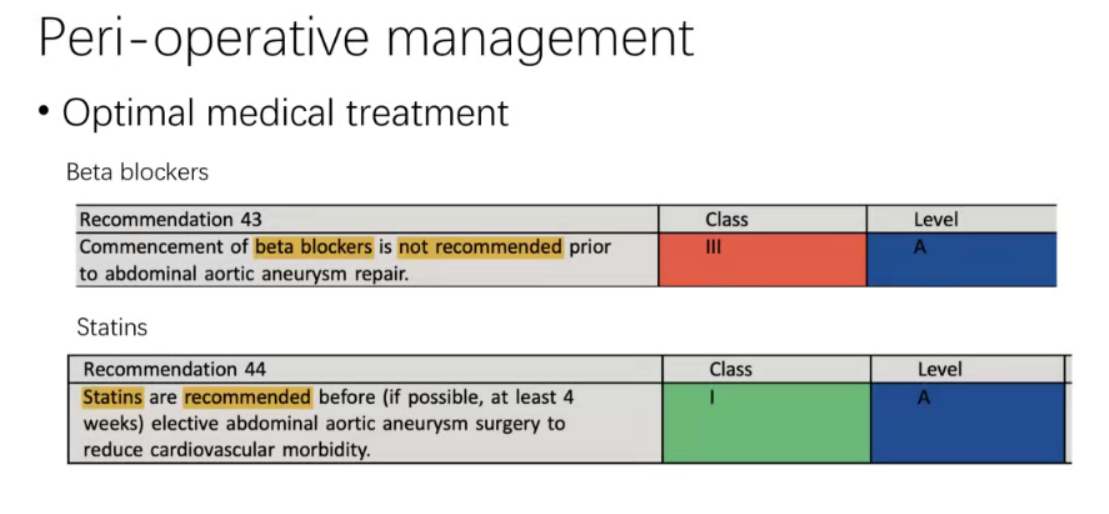
In the perioperative period, it is recommended that β-blockers and statins should be started immediately before repairing the abdominal aortic aneurysm to reduce the incidence of cardiovascular disease.
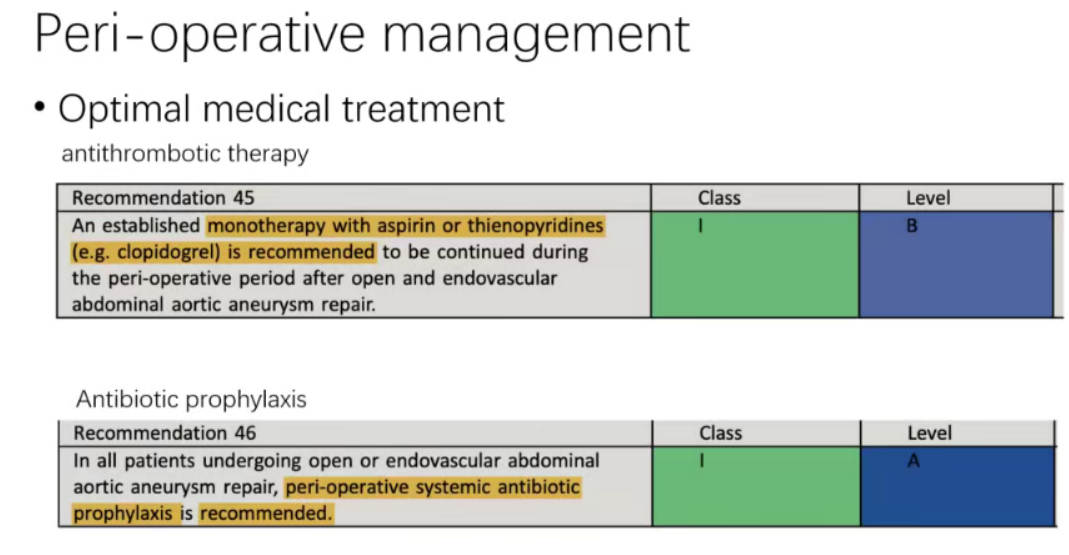
In terms of perioperative medical regimens, antithrombotic therapy, and in the perioperative period after open and endovascular abdominal aortic aneurysm repair, it is recommended to continue treatment with aspirin or clopidogrel. Perioperative systemic prophylactic antibiotics are also recommended for patients undergoing open or endovascular abdominal aortic aneurysm repair.
summary
1.Accurate measurement and preoperative planning are essential for early and long-term outcomes of EVAR postoperative success;
2. Preoperative and postoperative angiography provides important information for endovascular treatment of aortic disease;
3. Be proficient in endovascular techniques and follow streamlined surgical procedures to achieve fast, safe and effective results.
