

The "2022 Asian Endovascular Training Course (ATC)" was successfully held on November 22, 2022, Beijing time, sponsored by the National Center for Cardiovascular Diseases, undertaken by Fuwai Hospital Affiliated to the Chinese Academy of Sciences, with the China Vascular Congress as the academic support unit and the Hi Heart Voice Project Team as the media support unit.
The Asian Endovascular Training Course (ATC) program brings together many influential experts and scholars in Asia, with the purpose of "collaboration, communication, and improvement", in line with the principles of more scientific, authoritative, objective and practical, to convey the cutting-edge progress of cardiac surgery, inspire new ideas to overcome cardiac surgical diseases, provide a high-level platform for academic exchanges and learning, better assist clinicians in endovascular diagnosis and treatment, and provide strong support for clinical decision-making.
At the meeting, Professor Fang Kun from Fuwai Hospital, Chinese Academy of Medical Sciences, gave a wonderful speech on "TEVAR/EVAR Preoperative and Intraoperative Measurement and Evaluation Methods".
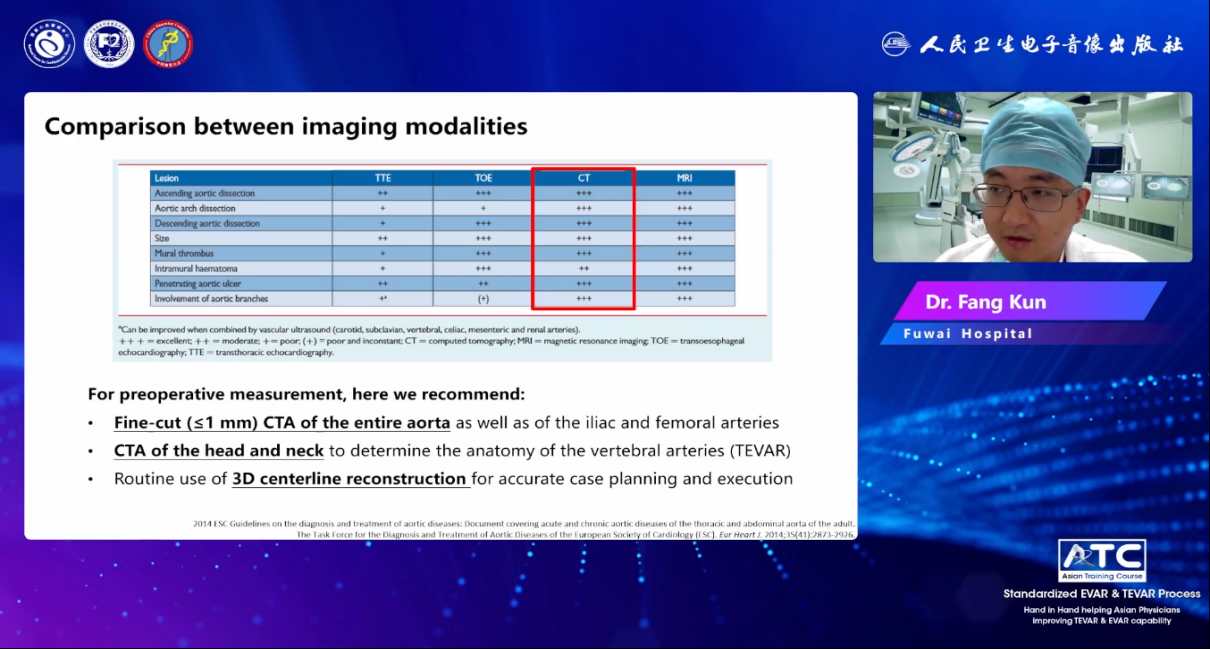
1.Comparison of different imaging tests
There are many imaging methods in the diagnosis and treatment of TEVAR/EVAR, such as TTE, TOE, CT, MRI, and Aortography, which comprehensively consider their advantages and disadvantages, such as ease of use, diagnostic reliability, bedside/interventional use, cost, radioactivity, etc. For preoperative measurements, CTAs are recommended in preference.
2.Preoperative and intraoperative evaluation of TEVAR
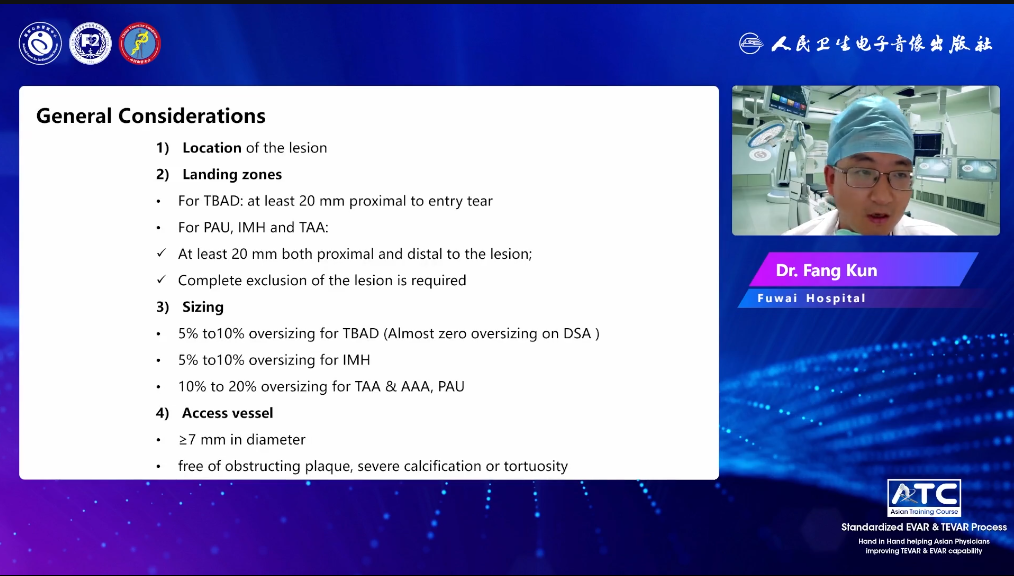
(1) The preoperative evaluation of TEVAR can generally be divided into four aspects:
1. Location of injury 2. Anchoring area①Type B aortic dissection (TABD): proximal break of at least 20mm②Penetrating aortic ulcer, thoracic aortic aneurysm, and aortic intermural hematoma: at least 20mm proximal and distal to the injury, 3. Size①Type B aortic dissection (TABD): the diameter of the prosthetic valve is greater than the diameter of the annulus 5%-10%②Aortic interwall hematoma (IMH): the diameter of the prosthetic valve is 5%-10% larger than the diameter of the annulus③Thoracic aortic aneurysm (TAA), penetrating aortic ulcer (PAU), abdominal aortic aneurysm (AAA): 10%-20% 4. The diameter of the radial vascular vessel is ≥7mm and there is no obstructive plaque, severe calcification or curvature.
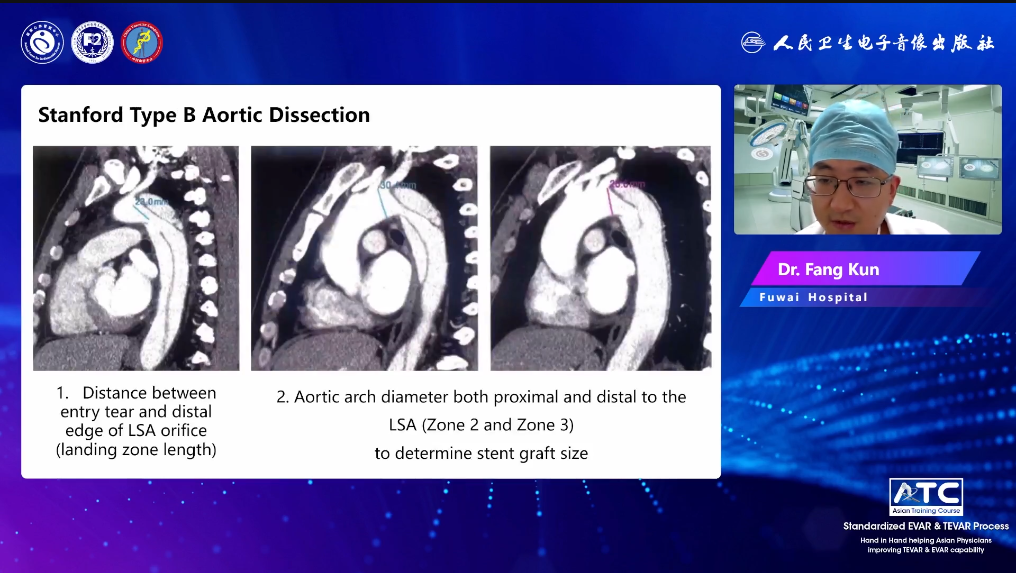
Type B interlayers need to be evaluated in many ways. The distance between the rupture and the left subclavian artery (LSA) determines the length of the anchoring area, and the diameter of the aortic arch, including the proximal and distal ends, and the distance from the LSA determines the size of the stent graft. In addition, the length of the long and short axes of different levels under imaging should be measured, and whether there is collateral involvement, poor perfusion, organ ischemia, etc. Look for signs of rupture, such as precursor rupture of aortic aneurysm, and total rupture.
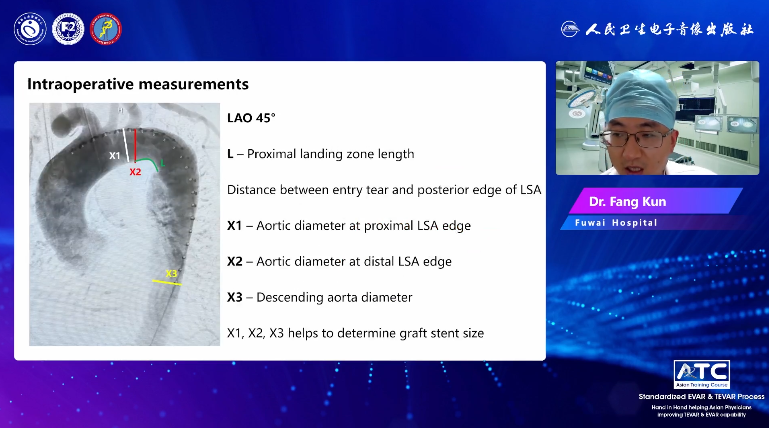
(2) Regarding TEVAR intraoperative evaluation.
The left anterior oblique position (LAO) of coronary angiography (LAO) 45°, the length of the proximal anchoring area, the distance between the rupture and the LSA opening, the diameter of the descending aorta, the diameter of the distal LSA marginal aorta, and the diameter of the proximal LSA marginal aorta determine the size of the stent graft.
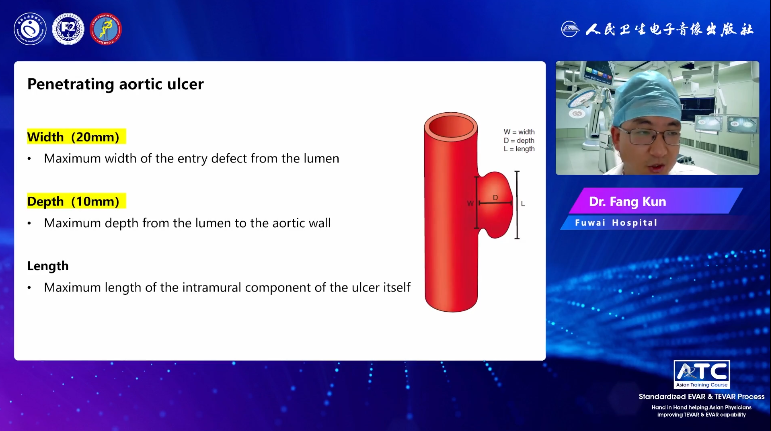
Penetrating aortic ulcer (PAU) is a focal ulcerative lesion that occurs in the area of atherosclerotic plaque that penetrates the elastic layer inside the blood vessel wall. In the treatment of PAU with TEVAR, it is generally necessary to evaluate the following: 1. the location of the injury, 2. whether there is an intramural hematoma, 3. peri-aortic tissue involvement, 4. peri-aortar hemorrhage, and 5. residual wall thickness. In addition, the maximum width of the rupture is 20 mm, the maximum depth from the lumen to the vessel wall is 10 mm, and the maximum length within the ulcer is its own size.
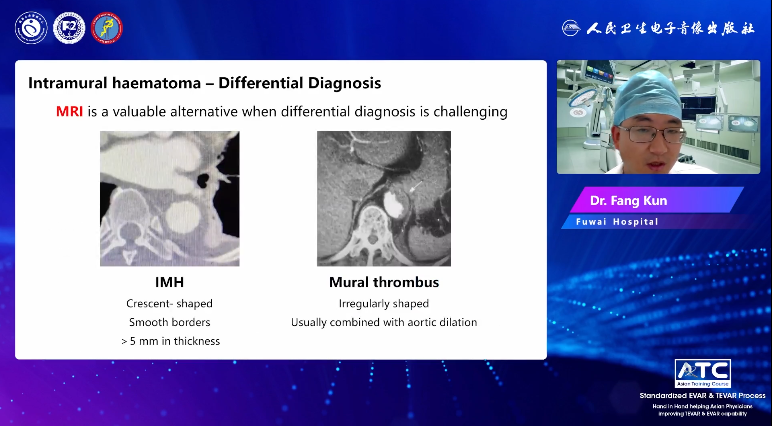
Preoperative imaging evaluation of intramural hematoma should include the location and extent of thickening of the vessel wall, which is round or crescent-shaped thickening of the aortic wall, ≥ 5 mm thick, and no significant blood flow. When it is difficult to diagnose with CTA, MRI with more diagnostic value can be selected to determine the spatial structure of the lesion site and aorta. For example, IMH is often differentiated from mural thrombosis, and the most typical and direct signs of IMH are crescent-shaped or annular thickening of the aortic wall ≥ 5 mm, and the inner wall of the adrenal thrombus is often irregular, and it is often combined with aortic dilation.
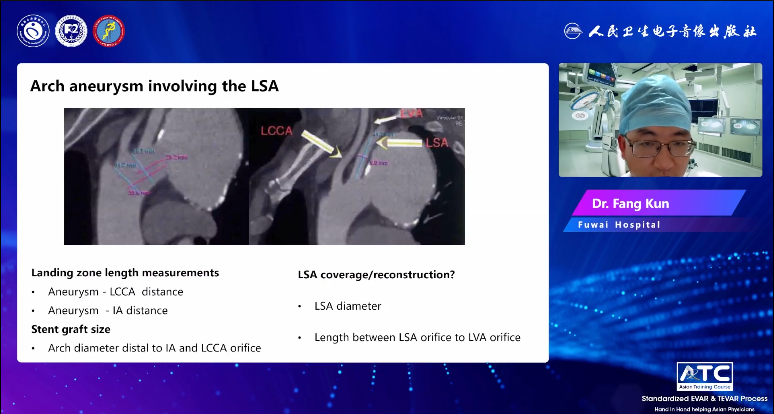
For arcuate aneurysms involving LSA, the length of the anchoring zone should be assessed based on the distance from the aneurysm to the LCCA (left common carotid artery) and IA. The size of the stent graft is determined by the diameter of the aortic arch distal to the lumen orifice of IA and LCCA. In addition, the choice of LSA for coverage or reconstruction is based on the evaluation of the diameter of the LSA and the length from the LSA orifice to the LVA orifice.
Preoperative and intraoperative evaluation of EVAR
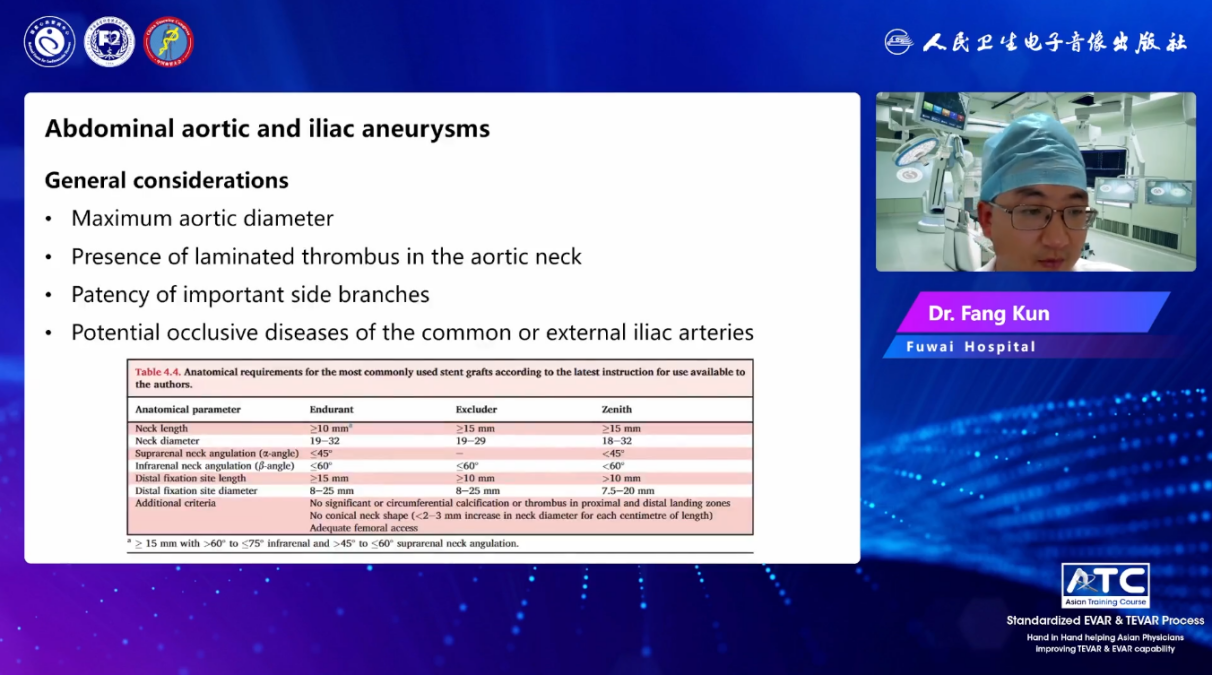
EVAR is effective in the treatment of abdominal aortic aneurysms and iliac artery aneurysms. In the preoperative and intraoperative evaluation, the maximum diameter of the aorta, the presence of aortic aneurysm cervical dissection thrombosis, the opening of important collateral circulation, and the potential common iliac artery or external iliac artery occlusive lesions should be evaluated.
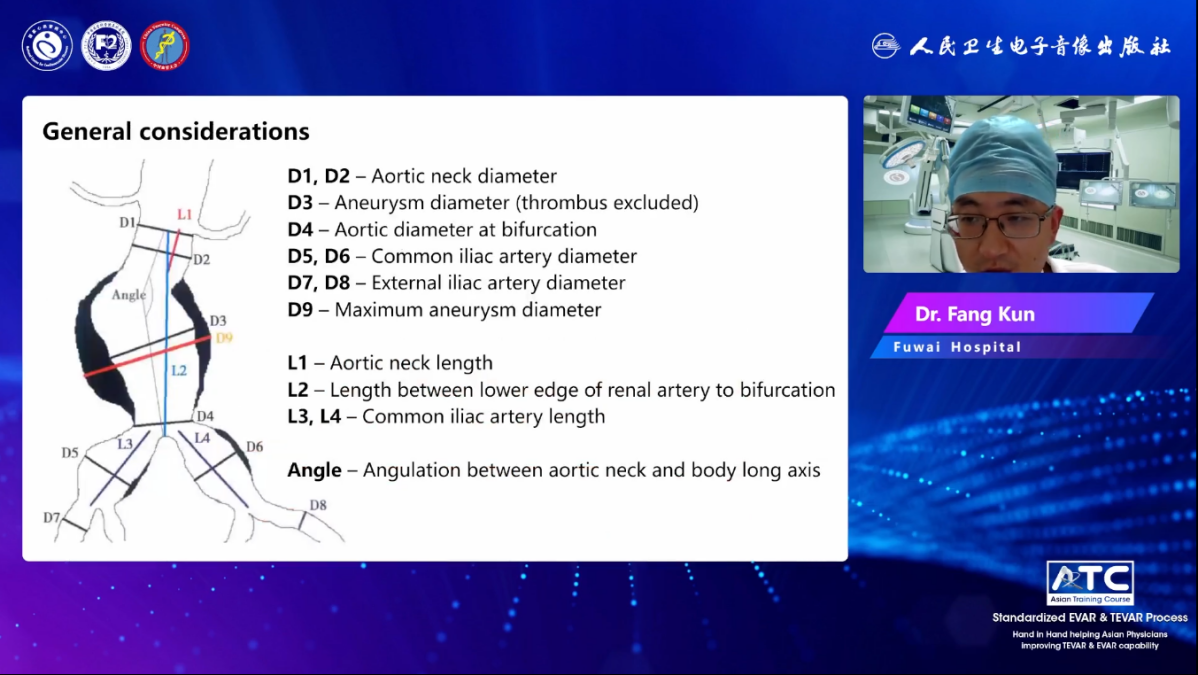
The general evaluation content is D1-D9, L1-L4 and angle, including aortic aneurysm neck diameter, maximum diameter of aortic aneurysm (excluding thrombus), aortic bifurcation diameter, common iliac artery diameter, external iliac artery diameter, aneurysm maximum diameter (including thrombosis), aneurysm neck length, lower renal artery to aortic bifurcation length, bilateral common iliac artery diameter, angle between aortic aneurysm neck and aneurysm long axis, etc.
In addition, it is important to note that complications affecting the visceral and collateral arteries, such as gluteal pain, claudication, sexual insufficiency, and intestinal ischemia, may occur after occlusion of the internal iliac artery. The diameter of the inferior mesenteric artery (IMA) and the number of lumbar arteries can affect the incidence of type II endoleak, and studies have shown that IMA diameter of ≥3 mm and/or 3 lumbar arteries ≥ open are high-risk factors for the development of type II endoleak.
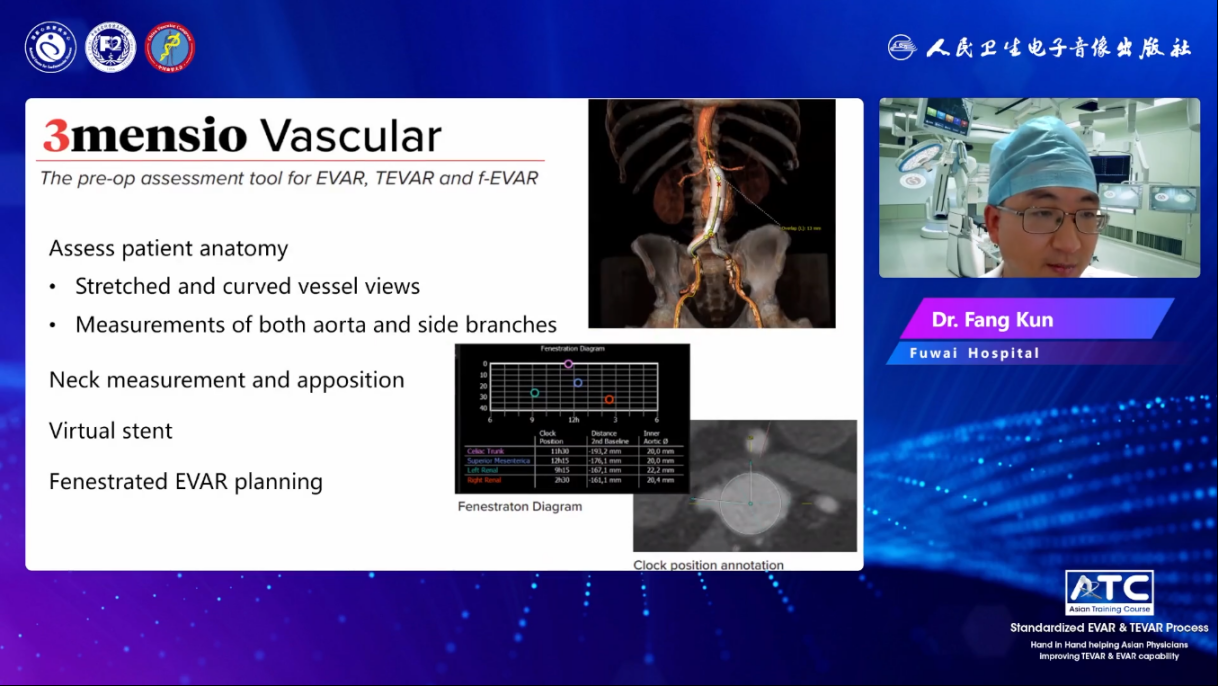
Preoperative evaluation software
The corresponding evaluation and measurement of EVAR, TEVAR, F-EVAR before surgery is inseparable from some advanced and practical software, such as 3mensio vascular CT, Endosize, etc. In clinical practice, the iterative and updated 3D navigation, 3D fusion, and 3D printing technologies are becoming more and more perfect, which is of great significance in the field of interventional surgery in vascular surgery.
Summary:
1.CTA is an effective and accurate preoperative measurement method;
2. Intraoperative DSA measurement can better and smoothly implant the device;
3. Relevant measurements should be taken with a thorough understanding of pathology;
4.3 mensio and Endosize are both powerful measurement tools;
5.3D navigation, 3D fusion, and 3D printing technologies have advantages in planning complex surgical plans.
